Diego Z Carvalho, Vaclav Kremen, Filip Mivalt, Erik K St Louis, Stuart J McCarter, Jan Bukartyk, Scott A Przybelski, Michael G Kamykowski, Anthony J Spychalla, Mary M Machulda, Bradley F Boeve, Ronald C Petersen, Clifford R Jack, Val J Lowe, Jonathan Graff-Radford, Gregory A Worrell, Virend K Somers, Andrew W Varga, Prashanthi Vemuri
{"title":"Non-rapid eye movement sleep slow-wave activity features are associated with amyloid accumulation in older adults with obstructive sleep apnoea.","authors":"Diego Z Carvalho, Vaclav Kremen, Filip Mivalt, Erik K St Louis, Stuart J McCarter, Jan Bukartyk, Scott A Przybelski, Michael G Kamykowski, Anthony J Spychalla, Mary M Machulda, Bradley F Boeve, Ronald C Petersen, Clifford R Jack, Val J Lowe, Jonathan Graff-Radford, Gregory A Worrell, Virend K Somers, Andrew W Varga, Prashanthi Vemuri","doi":"10.1093/braincomms/fcae354","DOIUrl":null,"url":null,"abstract":"<p><p>Obstructive sleep apnoea (OSA) is associated with an increased risk for cognitive impairment and dementia, which likely involves Alzheimer's disease pathology. Non-rapid eye movement slow-wave activity (SWA) has been implicated in amyloid clearance, but it has not been studied in the context of longitudinal amyloid accumulation in OSA. This longitudinal retrospective study aims to investigate the relationship between polysomnographic and electrophysiological SWA features and amyloid accumulation. From the Mayo Clinic Study of Aging cohort, we identified 71 participants ≥60 years old with OSA (mean baseline age = 72.9 ± 7.5 years, 60.6% male, 93% cognitively unimpaired) who had at least 2 consecutive Amyloid Pittsburgh Compound B (PiB)-PET scans and a polysomnographic study within 5 years of the baseline scan and before the second scan. Annualized PiB-PET accumulation [global ΔPiB(log)/year] was estimated by the difference between the second and first log-transformed global PiB-PET uptake estimations divided by the interval between scans (years). Sixty-four participants were included in SWA analysis. SWA was characterized by the mean relative spectral power density (%) in slow oscillation (SO: 0.5-0.9 Hz) and delta (1-3.9 Hz) frequency bands and by their downslopes (SO-slope and delta-slope, respectively) during the diagnostic portion of polysomnography. We fit linear regression models to test for associations among global ΔPiB(log)/year, SWA features (mean SO% and delta% or mean SO-slope and delta-slope), and OSA severity markers, after adjusting for age at baseline PiB-PET, <i>APOE ɛ4</i> and baseline amyloid positivity. For 1 SD increase in SO% and SO-slope, global ΔPiB(log)/year increased by 0.0033 (95% CI: 0.0001; 0.0064, <i>P</i> = 0.042) and 0.0069 (95% CI: 0.0009; 0.0129, <i>P</i> = 0.026), which were comparable to 32% and 59% of the effect size associated with baseline amyloid positivity, respectively. Delta-slope was associated with a reduction in global ΔPiB(log)/year by -0.0082 (95% CI: -0.0143; -0.0021, <i>P</i> = 0.009). Sleep apnoea severity was not associated with amyloid accumulation. Regional associations were stronger in the pre-frontal region. Both slow-wave slopes had more significant and widespread regional associations. Annualized PiB-PET accumulation was positively associated with SO and SO-slope, which may reflect altered sleep homeostasis due to increased homeostatic pressure in the setting of unmet sleep needs, increased synaptic strength, and/or hyper-excitability in OSA. Delta-slope was inversely associated with PiB-PET accumulation, suggesting it may represent residual physiological activity. Further investigation of SWA dynamics in the presence of sleep disorders before and after treatment is necessary for understanding the relationship between amyloid accumulation and SWA physiology.</p>","PeriodicalId":93915,"journal":{"name":"Brain communications","volume":"6 5","pages":"fcae354"},"PeriodicalIF":4.5000,"publicationDate":"2024-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11487750/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/braincomms/fcae354","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
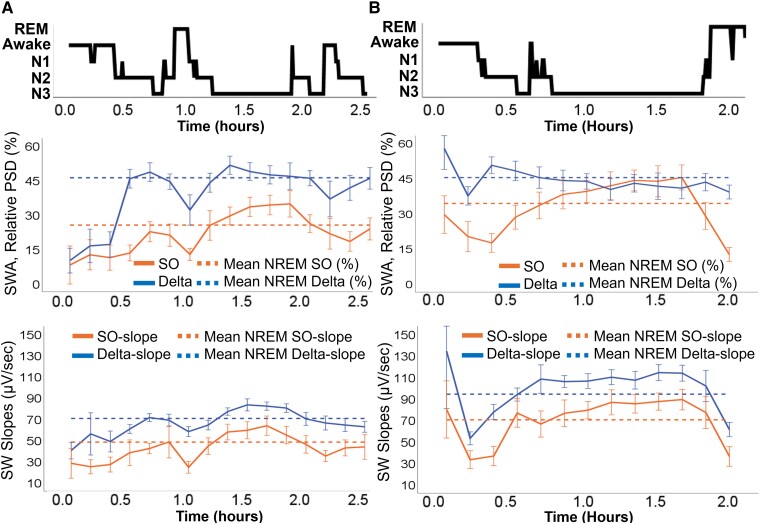
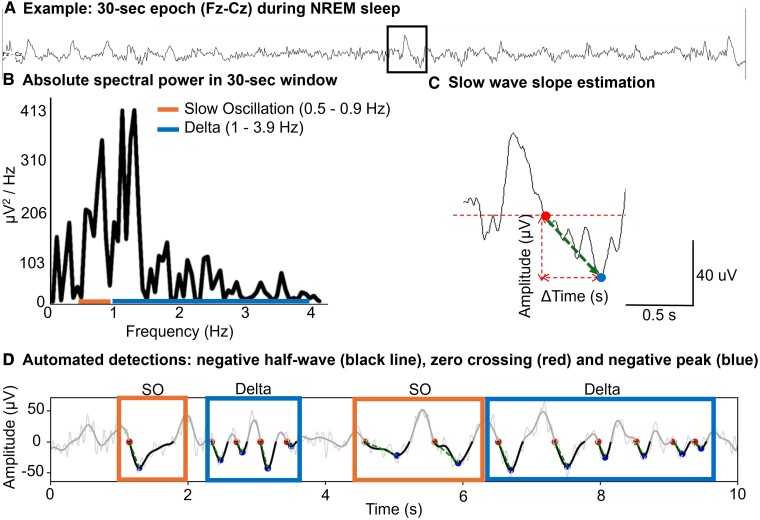
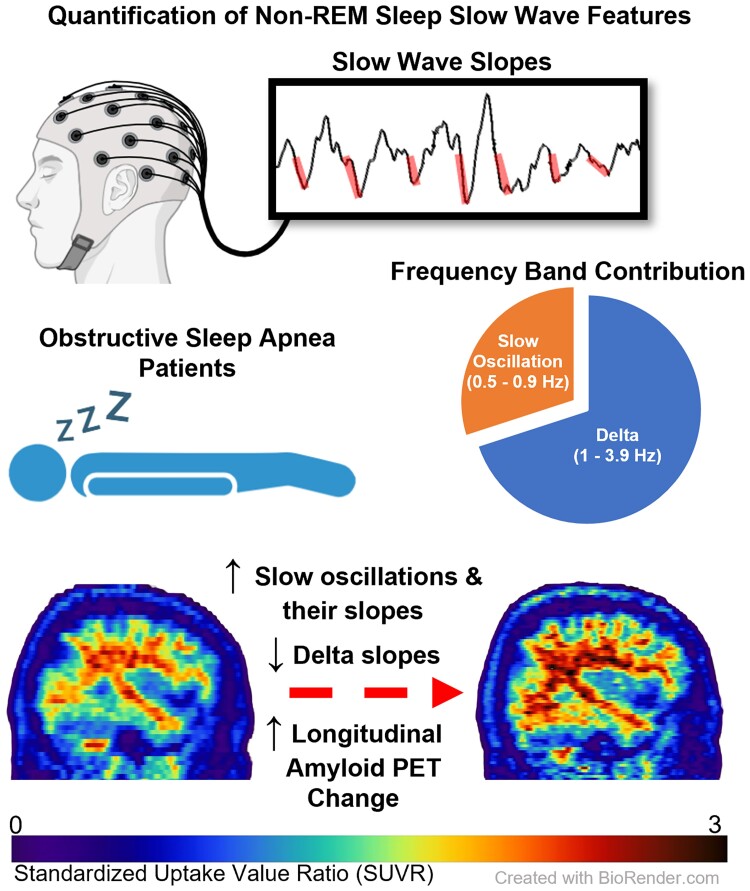
Obstructive sleep apnoea (OSA) is associated with an increased risk for cognitive impairment and dementia, which likely involves Alzheimer's disease pathology. Non-rapid eye movement slow-wave activity (SWA) has been implicated in amyloid clearance, but it has not been studied in the context of longitudinal amyloid accumulation in OSA. This longitudinal retrospective study aims to investigate the relationship between polysomnographic and electrophysiological SWA features and amyloid accumulation. From the Mayo Clinic Study of Aging cohort, we identified 71 participants ≥60 years old with OSA (mean baseline age = 72.9 ± 7.5 years, 60.6% male, 93% cognitively unimpaired) who had at least 2 consecutive Amyloid Pittsburgh Compound B (PiB)-PET scans and a polysomnographic study within 5 years of the baseline scan and before the second scan. Annualized PiB-PET accumulation [global ΔPiB(log)/year] was estimated by the difference between the second and first log-transformed global PiB-PET uptake estimations divided by the interval between scans (years). Sixty-four participants were included in SWA analysis. SWA was characterized by the mean relative spectral power density (%) in slow oscillation (SO: 0.5-0.9 Hz) and delta (1-3.9 Hz) frequency bands and by their downslopes (SO-slope and delta-slope, respectively) during the diagnostic portion of polysomnography. We fit linear regression models to test for associations among global ΔPiB(log)/year, SWA features (mean SO% and delta% or mean SO-slope and delta-slope), and OSA severity markers, after adjusting for age at baseline PiB-PET, APOE ɛ4 and baseline amyloid positivity. For 1 SD increase in SO% and SO-slope, global ΔPiB(log)/year increased by 0.0033 (95% CI: 0.0001; 0.0064, P = 0.042) and 0.0069 (95% CI: 0.0009; 0.0129, P = 0.026), which were comparable to 32% and 59% of the effect size associated with baseline amyloid positivity, respectively. Delta-slope was associated with a reduction in global ΔPiB(log)/year by -0.0082 (95% CI: -0.0143; -0.0021, P = 0.009). Sleep apnoea severity was not associated with amyloid accumulation. Regional associations were stronger in the pre-frontal region. Both slow-wave slopes had more significant and widespread regional associations. Annualized PiB-PET accumulation was positively associated with SO and SO-slope, which may reflect altered sleep homeostasis due to increased homeostatic pressure in the setting of unmet sleep needs, increased synaptic strength, and/or hyper-excitability in OSA. Delta-slope was inversely associated with PiB-PET accumulation, suggesting it may represent residual physiological activity. Further investigation of SWA dynamics in the presence of sleep disorders before and after treatment is necessary for understanding the relationship between amyloid accumulation and SWA physiology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
