{"title":"Management of Left Atrial Tachyrhythms in the Setting of HFpEF with Pulsed-Field Ablation: Treating Fire with Water?","authors":"Tyler Chinedu Chinyere, Ikeotunye Royal Chinyere","doi":"10.3390/therapeutics1010006","DOIUrl":null,"url":null,"abstract":"<p><p>Atrial fibrillation (AF) in the setting of heart failure (HF) with preserved ejection fraction (HFpEF) is a prevalent comorbidity and is enabled by adverse left atrial (LA) remodeling, dilation, and scar tissue formation. These changes are facilitated by poor left ventricular compliance. A growing body of clinical evidence and medical guidelines suggest that managing atrial tachyrhythms with catheter ablation (CA) is paramount to treating concomitant HF. This recommendation is complicated in that thermal CA modalities, namely radiofrequency ablation and cryoablation, are both therapeutic via inducing additional scar tissue. AF treatment with thermal CA may compound the atrial scar burden for patients who already have extensive scars secondary to HFpEF. Therefore, thermal CA could act as \"gasoline\" to the slowly burning \"fire\" within the LA, increasing the rate of AF recurrence. Pulsed-field ablation (PFA), which utilizes high-voltage irreversible electroporation, is a non-thermal CA technique that is capable of disrupting reentrant microcircuits and arrhythmogenic foci without inducing significant scar burden. PFA has the potential to mitigate the strong fibrosis response to thermal CA that predisposes to AF by serving as \"water\" rather than \"gasoline\". Thus, PFA may increase the efficacy and durability of CA for AF in HFpEF, and subsequently, may decrease the risk of procedural complications from repeat CAs. In this article, we provide a summary of the clinical concepts underlying HFpEF and AF and then summarize the data to date on the potential of PFA being a superior CA technique for AF in the setting of comorbid HFpEF.</p>","PeriodicalId":520250,"journal":{"name":"Therapeutics","volume":"1 1","pages":"42-51"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467807/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/therapeutics1010006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/23 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
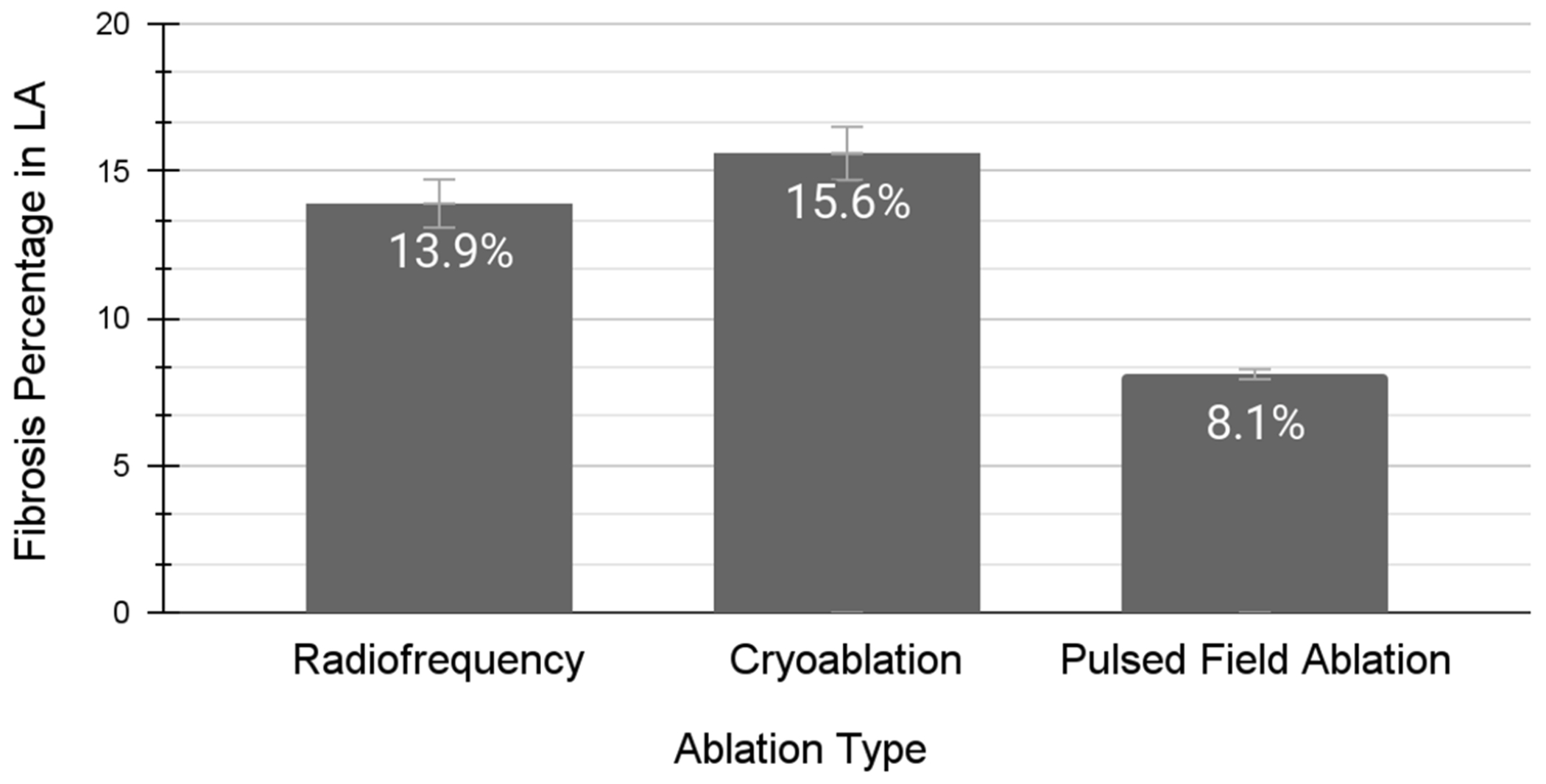
Atrial fibrillation (AF) in the setting of heart failure (HF) with preserved ejection fraction (HFpEF) is a prevalent comorbidity and is enabled by adverse left atrial (LA) remodeling, dilation, and scar tissue formation. These changes are facilitated by poor left ventricular compliance. A growing body of clinical evidence and medical guidelines suggest that managing atrial tachyrhythms with catheter ablation (CA) is paramount to treating concomitant HF. This recommendation is complicated in that thermal CA modalities, namely radiofrequency ablation and cryoablation, are both therapeutic via inducing additional scar tissue. AF treatment with thermal CA may compound the atrial scar burden for patients who already have extensive scars secondary to HFpEF. Therefore, thermal CA could act as "gasoline" to the slowly burning "fire" within the LA, increasing the rate of AF recurrence. Pulsed-field ablation (PFA), which utilizes high-voltage irreversible electroporation, is a non-thermal CA technique that is capable of disrupting reentrant microcircuits and arrhythmogenic foci without inducing significant scar burden. PFA has the potential to mitigate the strong fibrosis response to thermal CA that predisposes to AF by serving as "water" rather than "gasoline". Thus, PFA may increase the efficacy and durability of CA for AF in HFpEF, and subsequently, may decrease the risk of procedural complications from repeat CAs. In this article, we provide a summary of the clinical concepts underlying HFpEF and AF and then summarize the data to date on the potential of PFA being a superior CA technique for AF in the setting of comorbid HFpEF.
射血分数保留型心力衰竭(HF)时的心房颤动(AF)是一种普遍的合并症,其原因是左心房(LA)的重塑、扩张和瘢痕组织的形成。这些变化因左心室顺应性差而加剧。越来越多的临床证据和医疗指南表明,通过导管消融术(CA)控制房性心动过速对治疗合并高血压至关重要。这一建议比较复杂,因为热 CA 方式(即射频消融和冷冻消融)都是通过诱导额外的瘢痕组织来达到治疗目的的。使用热 CA 治疗房颤可能会加重心房瘢痕负担,因为患者已经因高频心房颤动而继发了广泛的瘢痕。因此,热CA可能会像 "汽油 "一样点燃LA内缓慢燃烧的 "火焰",从而增加房颤的复发率。脉冲场消融(PFA)利用高压不可逆电穿孔技术,是一种非热CA技术,能够破坏再入路微电路和致心律失常灶,而不会造成明显的疤痕负担。PFA 可作为 "水 "而不是 "汽油",从而减轻热 CA 所引起的强烈纤维化反应,这种反应容易导致房颤。因此,PFA 可提高 CA 治疗高频心衰房颤的疗效和耐久性,从而降低重复 CA 的手术并发症风险。在本文中,我们总结了 HFpEF 和房颤的基本临床概念,然后总结了迄今为止的数据,说明在合并 HFpEF 的情况下,PFA 有可能成为治疗房颤的一种卓越 CA 技术。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
