Christian Caillard, Emeline Fresnel, Elise Artaud-Macari, Antoine Cuvelier, Fabienne Tamion, Maxime Patout, Christophe Girault
{"title":"Ventilator performances for non-invasive ventilation: a bench study.","authors":"Christian Caillard, Emeline Fresnel, Elise Artaud-Macari, Antoine Cuvelier, Fabienne Tamion, Maxime Patout, Christophe Girault","doi":"10.1136/bmjresp-2023-002144","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>A wide range of recent ventilators, dedicated or not, is available for non-invasive ventilation (NIV) in respiratory or intensive care units (ICU). We conducted a bench study to compare their technical performances.</p><p><strong>Methods: </strong>Ventilators, including five ICU ventilators with NIV mode on, two dedicated NIV ventilators and one transport ventilator, were evaluated on a test bench for NIV, consisting of a 3D manikin head connected to an ASL 5000 lung model via a non-vented mask. Ventilators were tested according to three simulated lung profiles (normal, obstructive, restrictive), three levels of simulated air leakage (0, 15, 30 L/min), two levels of pressure support (8, 14 cmH<sub>2</sub>O) and two respiratory rates (15, 25 cycles/min).</p><p><strong>Results: </strong>The global median Asynchrony Index (AI) was higher with ICU ventilators than with dedicated NIV ventilators (4% (0; 76) vs 0% (0; 15), respectively; p<0.05) and different between all ventilators (p<0.001). The AI was higher with ICU ventilators for the normal and restrictive profiles (p<0.01) and not different between ventilators for the obstructive profile. Auto-triggering represented 43% of all patient-ventilator asynchrony. Triggering delay, cycling delay, inspiratory pressure-time product, pressure rise time and pressure at mask were different between all ventilators (p<0.01). Dedicated NIV ventilators induced a lower pressure-time product than ICU and transport ventilators (p<0.01). There was no difference between ventilators for minute ventilation and peak flow.</p><p><strong>Conclusion: </strong>Despite the integration of NIV algorithms, most recent ICU ventilators appear to be less efficient than dedicated NIV ventilators. Technical performances could change, however, according to the underlying respiratory disease and the level of air leakage.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"11 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499821/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2023-002144","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: A wide range of recent ventilators, dedicated or not, is available for non-invasive ventilation (NIV) in respiratory or intensive care units (ICU). We conducted a bench study to compare their technical performances.
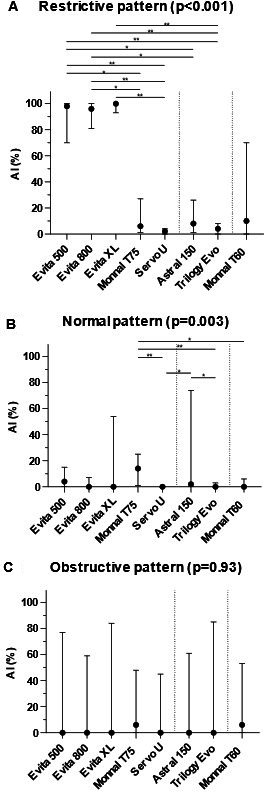
Methods: Ventilators, including five ICU ventilators with NIV mode on, two dedicated NIV ventilators and one transport ventilator, were evaluated on a test bench for NIV, consisting of a 3D manikin head connected to an ASL 5000 lung model via a non-vented mask. Ventilators were tested according to three simulated lung profiles (normal, obstructive, restrictive), three levels of simulated air leakage (0, 15, 30 L/min), two levels of pressure support (8, 14 cmH2O) and two respiratory rates (15, 25 cycles/min).
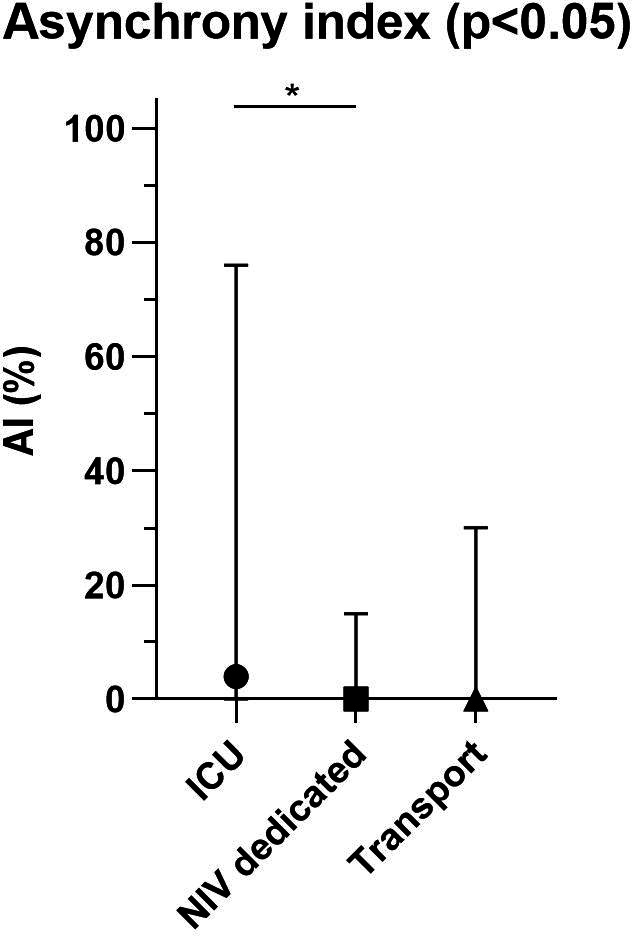
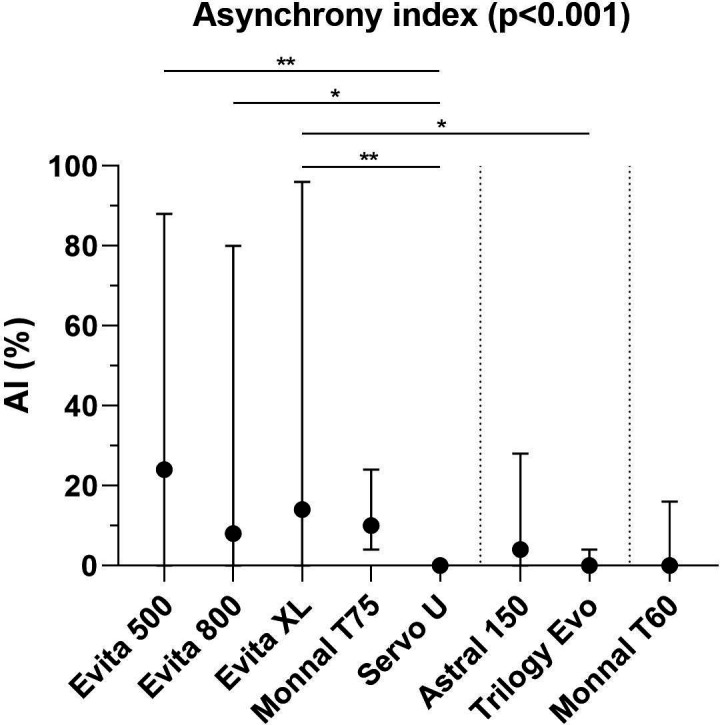
Results: The global median Asynchrony Index (AI) was higher with ICU ventilators than with dedicated NIV ventilators (4% (0; 76) vs 0% (0; 15), respectively; p<0.05) and different between all ventilators (p<0.001). The AI was higher with ICU ventilators for the normal and restrictive profiles (p<0.01) and not different between ventilators for the obstructive profile. Auto-triggering represented 43% of all patient-ventilator asynchrony. Triggering delay, cycling delay, inspiratory pressure-time product, pressure rise time and pressure at mask were different between all ventilators (p<0.01). Dedicated NIV ventilators induced a lower pressure-time product than ICU and transport ventilators (p<0.01). There was no difference between ventilators for minute ventilation and peak flow.
Conclusion: Despite the integration of NIV algorithms, most recent ICU ventilators appear to be less efficient than dedicated NIV ventilators. Technical performances could change, however, according to the underlying respiratory disease and the level of air leakage.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
