Cheng-Yang Hsieh, Po-Ting Chen, Shih-Chieh Shao, Swu-Jane Lin, Shu-Chen Liao, Edward Chia-Cheng Lai
{"title":"Validating ICD-10 Diagnosis Codes for Guillain-Barré Syndrome in Taiwan's National Health Insurance Claims Database.","authors":"Cheng-Yang Hsieh, Po-Ting Chen, Shih-Chieh Shao, Swu-Jane Lin, Shu-Chen Liao, Edward Chia-Cheng Lai","doi":"10.2147/CLEP.S485953","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To validate the International Classification of Diseases, 10th Revision (ICD-10) codes for Guillain-Barré syndrome (GBS) in Taiwan's insurance claims database.</p><p><strong>Methods: </strong>We identified adult patients hospitalized at any Chang Gung Memorial Foundation branch hospital between January 1st, 2017, and December 31st, 2022, with ICD-10 code G61.0 in any of the five discharge diagnosis positions, indicating possible Guillain-Barré syndrome. We then validated the possible GBS diagnosis using data from electronic medical records of the identified patients, based on the diagnostic criteria established by the National Institute of Neurological Disorders and Stroke. We determined the positive predictive values (PPV) of various operational definitions, including the position (primary or other) where the code was recorded in the discharge diagnosis, nerve conduction study (NCS) claims, and / or specific GBS treatments.</p><p><strong>Results: </strong>The final validation cohort of 484 patients with ICD-10 code for GBS in the discharge diagnosis was found to include 368 true GBS patients. Identifying inpatients using only the ICD-10 code for GBS in any of the five positions for discharge diagnosis yielded a PPV of 76.0%. With more restrictive definitions (primary diagnosis only, or requiring additional claims for NCS and/or treatments), the PPV tended to increase, but with fewer true GBS patients identified. Using ICD-10 GBS code in the primary diagnosis plus NCS and treatment claims yielded the highest PPV (98.3%); however, 140 (38.0%) of the true GBS patients were missed using this definition. In contrast, using the ICD-10 GBS code in any position, plus claims for NCS, achieved a relatively good PPV (85.8%) with minimal loss of true GBS patients (13, ie, 3.5%).</p><p><strong>Conclusion: </strong>In Taiwan's NHI claims data, identifying true GBS patients using only the ICD-10 code yielded a PPV of 76.0%; however, adding claims for diagnostic procedure and GBS treatment increased the PPV to 98.3%.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"16 ","pages":"733-742"},"PeriodicalIF":3.2000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11497080/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S485953","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To validate the International Classification of Diseases, 10th Revision (ICD-10) codes for Guillain-Barré syndrome (GBS) in Taiwan's insurance claims database.
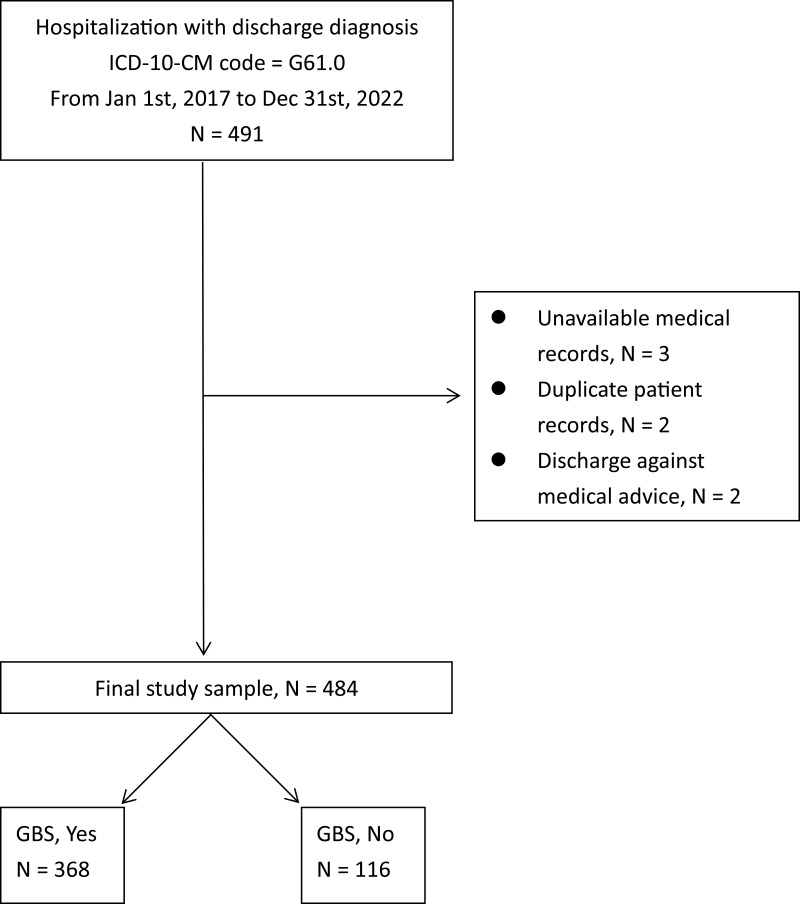
Methods: We identified adult patients hospitalized at any Chang Gung Memorial Foundation branch hospital between January 1st, 2017, and December 31st, 2022, with ICD-10 code G61.0 in any of the five discharge diagnosis positions, indicating possible Guillain-Barré syndrome. We then validated the possible GBS diagnosis using data from electronic medical records of the identified patients, based on the diagnostic criteria established by the National Institute of Neurological Disorders and Stroke. We determined the positive predictive values (PPV) of various operational definitions, including the position (primary or other) where the code was recorded in the discharge diagnosis, nerve conduction study (NCS) claims, and / or specific GBS treatments.
Results: The final validation cohort of 484 patients with ICD-10 code for GBS in the discharge diagnosis was found to include 368 true GBS patients. Identifying inpatients using only the ICD-10 code for GBS in any of the five positions for discharge diagnosis yielded a PPV of 76.0%. With more restrictive definitions (primary diagnosis only, or requiring additional claims for NCS and/or treatments), the PPV tended to increase, but with fewer true GBS patients identified. Using ICD-10 GBS code in the primary diagnosis plus NCS and treatment claims yielded the highest PPV (98.3%); however, 140 (38.0%) of the true GBS patients were missed using this definition. In contrast, using the ICD-10 GBS code in any position, plus claims for NCS, achieved a relatively good PPV (85.8%) with minimal loss of true GBS patients (13, ie, 3.5%).
Conclusion: In Taiwan's NHI claims data, identifying true GBS patients using only the ICD-10 code yielded a PPV of 76.0%; however, adding claims for diagnostic procedure and GBS treatment increased the PPV to 98.3%.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
