Cost-Effectiveness of Empagliflozin (JARDIANCE®) in the Treatment of Patients with Chronic Kidney Disease in France, Based on the EMPA-KIDNEY Clinical Trial.
Harinala Groyer, Romain Supiot, Jean Tardu, Nicolas Virely, Marine Sivignon, Denis San, Pierre Lévy, Anastasia Ustyugova, Ziad A Massy
{"title":"Cost-Effectiveness of Empagliflozin (JARDIANCE<sup>®</sup>) in the Treatment of Patients with Chronic Kidney Disease in France, Based on the EMPA-KIDNEY Clinical Trial.","authors":"Harinala Groyer, Romain Supiot, Jean Tardu, Nicolas Virely, Marine Sivignon, Denis San, Pierre Lévy, Anastasia Ustyugova, Ziad A Massy","doi":"10.1007/s40261-024-01398-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>The efficacy and safety of empagliflozin in the treatment of chronic kidney disease (CKD) were demonstrated in the EMPA-KIDNEY trial, which showed a 28% reduction in combined risks of kidney disease or death from cardiovascular causes (hazard ratio, 0.72; 95% confidence interval, 0.64-0.82; p < 0.001) compared with placebo. Based on these results, the present study aimed to assess the cost-effectiveness of empagliflozin + standard of care (SoC) compared with SoC alone in the treatment of CKD in France.</p><p><strong>Methods: </strong>A Markov state microsimulation model was adapted to compare the health and economic outcomes in France, considering a healthcare system perspective, in patients treated with empagliflozin in addition to SoC versus patients treated with SoC alone. The model simulated the intention-to-treat population of the trial, transitioning between 18 mutually exclusive and collectively exhaustive health states defined based on the Kidney Disease: Improving Global Outcomes classification. For each arm, the model estimated (over a 25-year time horizon) the number of events and deaths, and the costs associated with these events, to calculate the incremental cost-effectiveness ratio. The resources used were derived using French authorities reports, literature, and French CKD guidelines. Both economic and health outcomes were discounted at a 2.5% annual rate according to French guidelines.</p><p><strong>Results: </strong>The model predicted that using empagliflozin + SoC to treat patients with CKD would prevent CKD-related complications and deaths associated with a cardiovascular event or all-cause deaths while in kidney replacement therapy, resulting on average in a discounted gain of 1.29 years in overall survival (9.48 years vs. 8.19 with SoC alone). Empagliflozin costs (treatment, events, and disease management) were completely offset by the cost savings from avoided kidney failure events. Overall, empagliflozin + SoC would be more effective and less costly than SoC alone and would therefore be the dominant treatment strategy. The sensitivity analyses conducted support the results' robustness in showing the dominance of empagliflozin + SoC over SoC alone.</p><p><strong>Conclusions: </strong>The base-case results indicate that empagliflozin + SoC is a dominant strategy compared with the current SoC for the management of CKD in France. Empagliflozin + SoC would have a positive impact on patients with CKD by slowing CKD progression and leading to the prevention of kidney failure events on top of all-stages CKD complications.</p>","PeriodicalId":10402,"journal":{"name":"Clinical Drug Investigation","volume":" ","pages":"811-828"},"PeriodicalIF":2.7000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11564328/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Drug Investigation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40261-024-01398-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
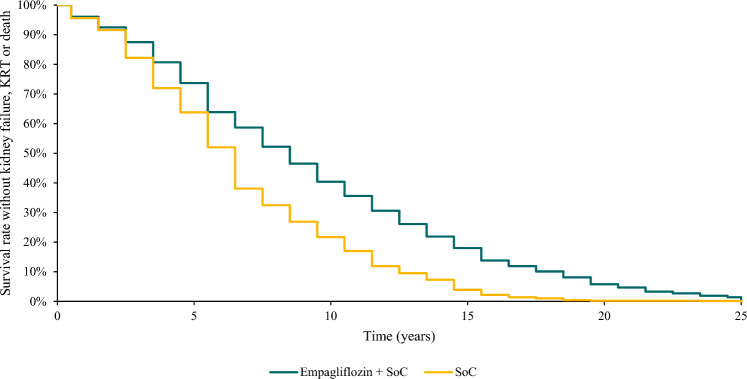
Background and objective: The efficacy and safety of empagliflozin in the treatment of chronic kidney disease (CKD) were demonstrated in the EMPA-KIDNEY trial, which showed a 28% reduction in combined risks of kidney disease or death from cardiovascular causes (hazard ratio, 0.72; 95% confidence interval, 0.64-0.82; p < 0.001) compared with placebo. Based on these results, the present study aimed to assess the cost-effectiveness of empagliflozin + standard of care (SoC) compared with SoC alone in the treatment of CKD in France.
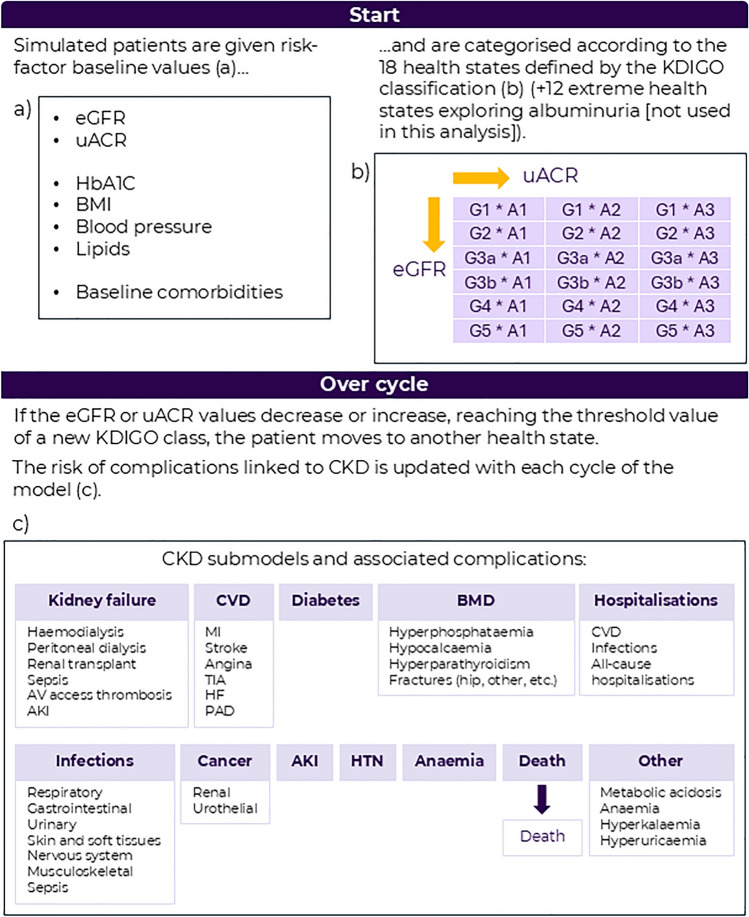
Methods: A Markov state microsimulation model was adapted to compare the health and economic outcomes in France, considering a healthcare system perspective, in patients treated with empagliflozin in addition to SoC versus patients treated with SoC alone. The model simulated the intention-to-treat population of the trial, transitioning between 18 mutually exclusive and collectively exhaustive health states defined based on the Kidney Disease: Improving Global Outcomes classification. For each arm, the model estimated (over a 25-year time horizon) the number of events and deaths, and the costs associated with these events, to calculate the incremental cost-effectiveness ratio. The resources used were derived using French authorities reports, literature, and French CKD guidelines. Both economic and health outcomes were discounted at a 2.5% annual rate according to French guidelines.
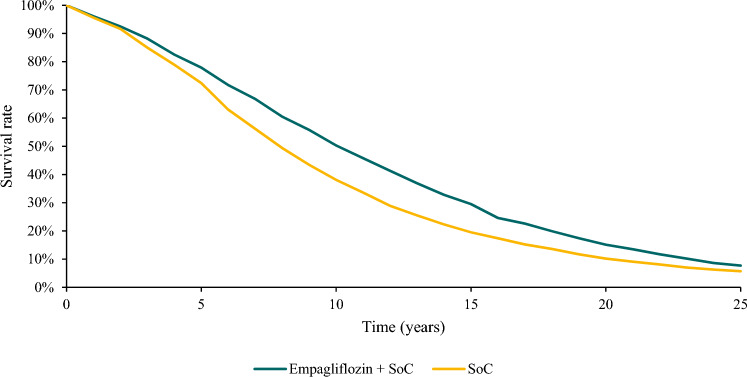
Results: The model predicted that using empagliflozin + SoC to treat patients with CKD would prevent CKD-related complications and deaths associated with a cardiovascular event or all-cause deaths while in kidney replacement therapy, resulting on average in a discounted gain of 1.29 years in overall survival (9.48 years vs. 8.19 with SoC alone). Empagliflozin costs (treatment, events, and disease management) were completely offset by the cost savings from avoided kidney failure events. Overall, empagliflozin + SoC would be more effective and less costly than SoC alone and would therefore be the dominant treatment strategy. The sensitivity analyses conducted support the results' robustness in showing the dominance of empagliflozin + SoC over SoC alone.
Conclusions: The base-case results indicate that empagliflozin + SoC is a dominant strategy compared with the current SoC for the management of CKD in France. Empagliflozin + SoC would have a positive impact on patients with CKD by slowing CKD progression and leading to the prevention of kidney failure events on top of all-stages CKD complications.
期刊介绍:
Clinical Drug Investigation provides rapid publication of original research covering all phases of clinical drug development and therapeutic use of drugs. The Journal includes:
-Clinical trials, outcomes research, clinical pharmacoeconomic studies and pharmacoepidemiology studies with a strong link to optimum prescribing practice for a drug or group of drugs.
-Clinical pharmacodynamic and clinical pharmacokinetic studies with a strong link to clinical practice.
-Pharmacodynamic and pharmacokinetic studies in healthy volunteers in which significant implications for clinical prescribing are discussed.
-Studies focusing on the application of drug delivery technology in healthcare.
-Short communications and case study reports that meet the above criteria will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Clinical Drug Investigation may be accompanied by plain language summaries to assist readers who have some knowledge, but non in-depth expertise in, the area to understand important medical advances.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
