Sonya M Jampel, Joel Kaufman, Daniel A Enquobahrie, Adrien A Wilkie, Amanda J Gassett, Thomas J Luben
{"title":"Association between fine particulate matter (PM<sub>2.5</sub>) and infant mortality in a North Carolina birth cohort (2003-2015).","authors":"Sonya M Jampel, Joel Kaufman, Daniel A Enquobahrie, Adrien A Wilkie, Amanda J Gassett, Thomas J Luben","doi":"10.1097/EE9.0000000000000350","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While the association between fine particulate matter (PM<sub>2.5</sub>) and adult mortality is well established, few studies have examined the association between long-term PM<sub>2.5</sub> exposure and infant mortality.</p><p><strong>Methods: </strong>We conducted an unmatched case-control study of 5992 infant mortality cases and 60,000 randomly selected controls from a North Carolina birth cohort (2003-2015). PM<sub>2.5</sub> during critical exposure periods (trimesters, pregnancy, first month alive) was estimated using residential address and a national spatiotemporal model at census block centroid. We fit adjusted logistic regression models and calculated odds ratios (ORs) and 95% confidence intervals (CIs). Due to differences in PM<sub>2</sub> <sub>.5</sub> over time, we stratified analyses into two periods: 2003-2009 (mean = 12.1 µg/m<sup>3</sup>, interquartile range [IQR]: 10.8-13.5) and 2011-2015 (mean = 8.4 µg/m<sup>3</sup>, IQR: 7.7-9.0). We assessed effect measure modification by birthing parent race/ethnicity, full-term birth, and PM<sub>2.5</sub> concentrations.</p><p><strong>Results: </strong>For births 2003-2015, the odds of infant mortality increased by 12% (95% CI: 1.06, 1.17) per 4.0 µg/m<sup>3</sup> increase in PM<sub>2.5</sub> exposure averaged over the pregnancy. After stratifying, we observed an increase of 4% (95% CI: 0.95, 1.14) for births in 2003-2009 and a decrease of 15% (95% CI: 0.72, 1.01) for births in 2011-2015. Among infants with higher PM<sub>2.5</sub> exposure (≥12 µg/m<sup>3</sup>) during pregnancy, the odds of infant mortality increased (OR: 2.69; 95% CI: 2.17, 3.34) whereas the lower exposure (<8 µg/m<sup>3</sup>) group reported decreased odds (OR: 0.50; 95% CI: 0.28, 0.89).</p><p><strong>Conclusions: </strong>We observed differing associations of PM<sub>2.5</sub> exposure with infant mortality across higher versus lower PM<sub>2.5</sub> concentrations. Research findings suggest the importance of accounting for long-term trends of decreasing PM<sub>2.5</sub> concentrations in future research.</p>","PeriodicalId":11713,"journal":{"name":"Environmental Epidemiology","volume":"8 6","pages":"e350"},"PeriodicalIF":3.8000,"publicationDate":"2024-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11512634/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Environmental Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/EE9.0000000000000350","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENVIRONMENTAL SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: While the association between fine particulate matter (PM2.5) and adult mortality is well established, few studies have examined the association between long-term PM2.5 exposure and infant mortality.
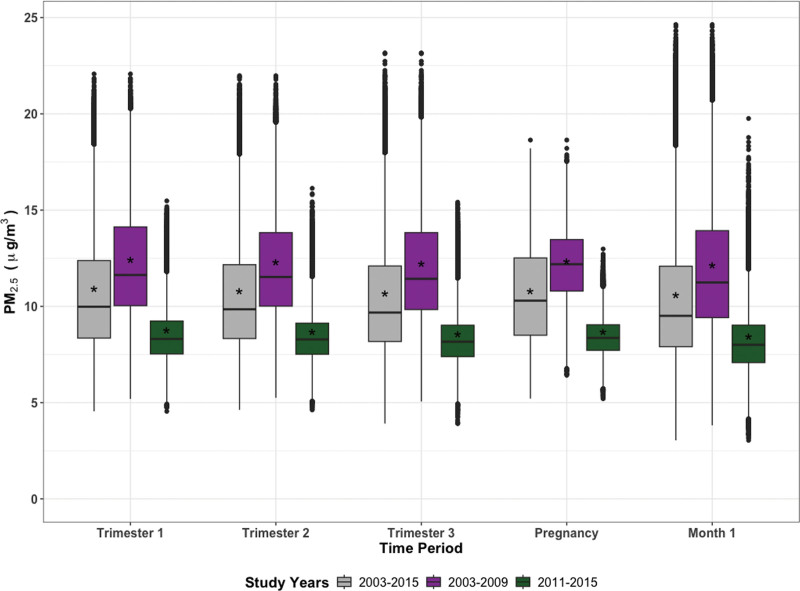
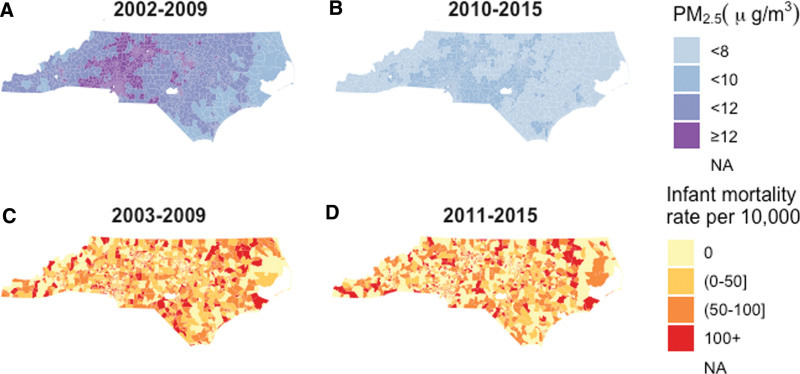
Methods: We conducted an unmatched case-control study of 5992 infant mortality cases and 60,000 randomly selected controls from a North Carolina birth cohort (2003-2015). PM2.5 during critical exposure periods (trimesters, pregnancy, first month alive) was estimated using residential address and a national spatiotemporal model at census block centroid. We fit adjusted logistic regression models and calculated odds ratios (ORs) and 95% confidence intervals (CIs). Due to differences in PM2.5 over time, we stratified analyses into two periods: 2003-2009 (mean = 12.1 µg/m3, interquartile range [IQR]: 10.8-13.5) and 2011-2015 (mean = 8.4 µg/m3, IQR: 7.7-9.0). We assessed effect measure modification by birthing parent race/ethnicity, full-term birth, and PM2.5 concentrations.
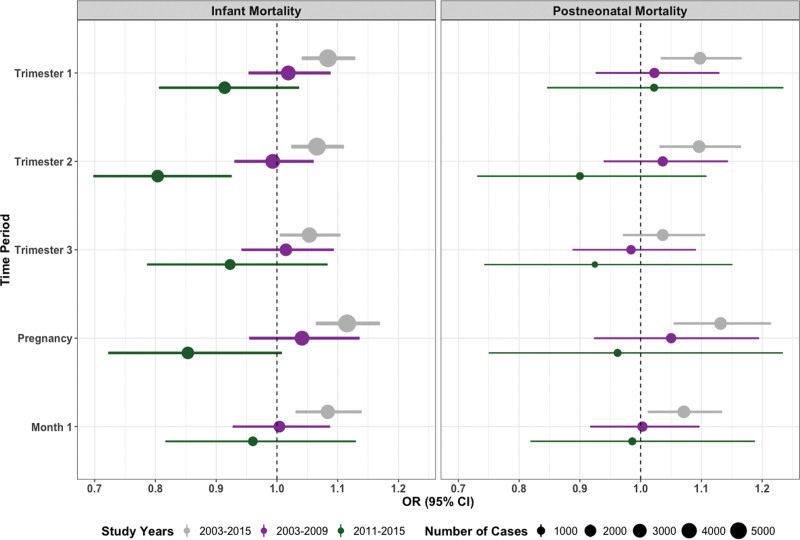
Results: For births 2003-2015, the odds of infant mortality increased by 12% (95% CI: 1.06, 1.17) per 4.0 µg/m3 increase in PM2.5 exposure averaged over the pregnancy. After stratifying, we observed an increase of 4% (95% CI: 0.95, 1.14) for births in 2003-2009 and a decrease of 15% (95% CI: 0.72, 1.01) for births in 2011-2015. Among infants with higher PM2.5 exposure (≥12 µg/m3) during pregnancy, the odds of infant mortality increased (OR: 2.69; 95% CI: 2.17, 3.34) whereas the lower exposure (<8 µg/m3) group reported decreased odds (OR: 0.50; 95% CI: 0.28, 0.89).
Conclusions: We observed differing associations of PM2.5 exposure with infant mortality across higher versus lower PM2.5 concentrations. Research findings suggest the importance of accounting for long-term trends of decreasing PM2.5 concentrations in future research.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
