Silvia Mongodi, Davide Chiumello, Francesco Mojoli
{"title":"Lung ultrasound score for the assessment of lung aeration in ARDS patients: comparison of two approaches.","authors":"Silvia Mongodi, Davide Chiumello, Francesco Mojoli","doi":"10.1055/a-2421-8709","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose</b> A 4-step lung ultrasound (LUS) score has been previously used to quantify lung density. We compared 2 versions of this scoring system for distinguishing severe from moderate loss of aeration in ARDS: coalescence-based score (cLUS) vs. quantitative-based score (qLUS - >50% pleura occupied by artefacts). <b>Materials and Methods</b> We compared qLUS and cLUS to lung density measured by quantitative CT scan in 12 standard thoracic regions. A simplified approach (1 scan per region) was compared to an extensive one (regional score computed as the mean of all relevant intercostal space scores). <b>Results</b> We examined 13 conditions in 7 ARDS patients (7 at PEEP 5, 6 at PEEP 15 cmH2O-156 regions, 398 clips). Switching from cLUS to qLUS resulted in a change in interpretation in 117 clips (29.4%, 1-point reduction) and in 41.7% of the regions (64 decreases (range 0.2-1), 1 increase (0.2 points)). Regional qLUS showed very strong correlation with lung density (rs=0.85), higher than cLUS (rs=0.79; p=0.010). The agreement with CT classification in well aerated, poorly aerated, and not aerated tissue was moderate for cLUS (agreement 65.4%; Cohen's K coefficient 0.475 (95%CI 0.391-0.547); p<0.0001) and substantial for qLUS (agreement 81.4%; Cohen's K coefficient 0.701 (95%CI 0.653-0.765), p<0.0001). The agreement between single spot and extensive approaches was almost perfect (cLUS: agreement 89.1%, Cohen's kappa coefficient 0.840 (95%CI 0.811-0.911), p<0.0001; qLUS: agreement 86.5%, Cohen's kappa coefficient 0.819 (95%CI 0.761-0.848), p<0.0001). <b>Conclusion</b> A LUS score based on the percentage of occupied pleura performs better than a coalescence-based approach for quantifying lung density. A simplified approach performs as well as an extensive one.</p>","PeriodicalId":44852,"journal":{"name":"Ultrasound International Open","volume":"10 ","pages":"a24218709"},"PeriodicalIF":1.6000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11497101/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2421-8709","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
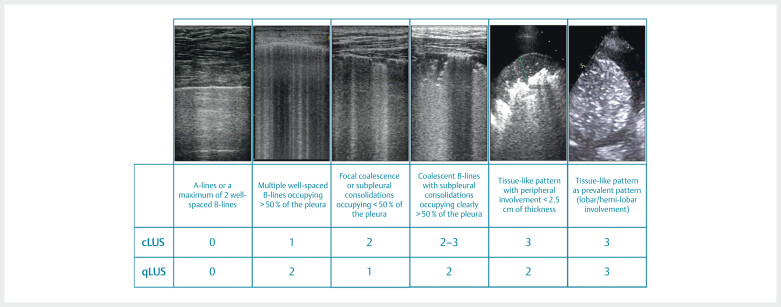
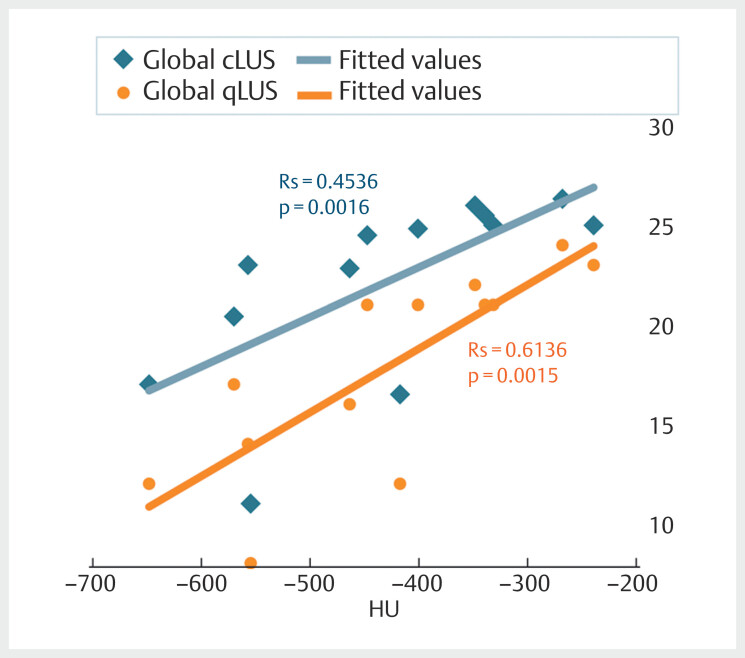
Purpose A 4-step lung ultrasound (LUS) score has been previously used to quantify lung density. We compared 2 versions of this scoring system for distinguishing severe from moderate loss of aeration in ARDS: coalescence-based score (cLUS) vs. quantitative-based score (qLUS - >50% pleura occupied by artefacts). Materials and Methods We compared qLUS and cLUS to lung density measured by quantitative CT scan in 12 standard thoracic regions. A simplified approach (1 scan per region) was compared to an extensive one (regional score computed as the mean of all relevant intercostal space scores). Results We examined 13 conditions in 7 ARDS patients (7 at PEEP 5, 6 at PEEP 15 cmH2O-156 regions, 398 clips). Switching from cLUS to qLUS resulted in a change in interpretation in 117 clips (29.4%, 1-point reduction) and in 41.7% of the regions (64 decreases (range 0.2-1), 1 increase (0.2 points)). Regional qLUS showed very strong correlation with lung density (rs=0.85), higher than cLUS (rs=0.79; p=0.010). The agreement with CT classification in well aerated, poorly aerated, and not aerated tissue was moderate for cLUS (agreement 65.4%; Cohen's K coefficient 0.475 (95%CI 0.391-0.547); p<0.0001) and substantial for qLUS (agreement 81.4%; Cohen's K coefficient 0.701 (95%CI 0.653-0.765), p<0.0001). The agreement between single spot and extensive approaches was almost perfect (cLUS: agreement 89.1%, Cohen's kappa coefficient 0.840 (95%CI 0.811-0.911), p<0.0001; qLUS: agreement 86.5%, Cohen's kappa coefficient 0.819 (95%CI 0.761-0.848), p<0.0001). Conclusion A LUS score based on the percentage of occupied pleura performs better than a coalescence-based approach for quantifying lung density. A simplified approach performs as well as an extensive one.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
