Rezafungin versus caspofungin for patients with candidaemia or invasive candidiasis in the intensive care unit: pooled analyses of the ReSTORE and STRIVE randomised trials.
Patrick M Honoré, Massimo Girardis, Marin Kollef, Oliver A Cornely, George R Thompson, Matteo Bassetti, Alex Soriano, Haihui Huang, Jose Vazquez, Bart Jan Kullberg, Peter G Pappas, Nick Manamley, Taylor Sandison, John Pullman, Saad Nseir
{"title":"Rezafungin versus caspofungin for patients with candidaemia or invasive candidiasis in the intensive care unit: pooled analyses of the ReSTORE and STRIVE randomised trials.","authors":"Patrick M Honoré, Massimo Girardis, Marin Kollef, Oliver A Cornely, George R Thompson, Matteo Bassetti, Alex Soriano, Haihui Huang, Jose Vazquez, Bart Jan Kullberg, Peter G Pappas, Nick Manamley, Taylor Sandison, John Pullman, Saad Nseir","doi":"10.1186/s13054-024-05117-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rezafungin is an echinocandin approved in the US and EU to treat candidaemia and/or invasive candidiasis. This post-hoc, pooled analysis of the Phase 2 STRIVE and Phase 3 ReSTORE trials assessed rezafungin versus caspofungin in patients with candidaemia and/or invasive candidiasis (IC) in the intensive care unit (ICU) at randomisation.</p><p><strong>Methods: </strong>STRIVE and ReSTORE were randomised double-blind trials in adults with systemic signs and mycological confirmation of candidaemia and/or IC in blood or a normally sterile site ≤ 96 h before randomisation. Data were pooled for patients in the ICU at randomisation who received intravenous rezafungin (400 mg loading dose then 200 mg once weekly) or caspofungin (70 mg loading dose then 50 mg once daily) for ≤ 4 weeks. Outcomes were Day 30 all-cause mortality (primary outcome), Day 5 and 14 mycological eradication, time to negative blood culture, mortality attributable to candidaemia/invasive candidiasis, safety, and pharmacokinetics.</p><p><strong>Results: </strong>Of 294 patients in STRIVE/ReSTORE, 113 were in the ICU at randomisation (rezafungin n = 46; caspofungin n = 67). At baseline, ~ 30% of patients in each group had impaired renal function and/or an Acute Physiologic Assessment and Chronic Health Evaluation II score ≥ 20. One patient (in the caspofungin group) was neutropenic at baseline. Day 30 all-cause mortality was 34.8% for rezafungin versus 25.4% for caspofungin. Day 5 and 14 mycological eradication was 78.3% and 71.7% for rezafungin versus 59.7% and 65.7% for caspofungin, respectively. Median time to negative blood culture was 18 (interquartile range, 12.6-43.0) versus 38 (interquartile range, 15.9-211.3) h for rezafungin versus caspofungin (stratified log-rank P = 0.001; nominal, not adjusted for multiplicity). Candidaemia/IC-attributable deaths occurred in two rezafungin patients versus one caspofungin patient. Safety profiles were similar between groups. Overall, 17.4% (rezafungin) versus 29.9% (caspofungin) of patients discontinued due to treatment-emergent adverse events. Rezafungin exposure following the initial 400-mg dose was comparable between patients in the ICU at randomisation (n = 50) and non-ICU patients (n = 117).</p><p><strong>Conclusions: </strong>Rezafungin was well tolerated and efficacious in critically ill, mainly non-neutropenic patients with candidaemia and/or IC. This analysis provides additional insights into the efficacy and safety of rezafungin in the ICU population.</p>","PeriodicalId":10811,"journal":{"name":"Critical Care","volume":"28 1","pages":"348"},"PeriodicalIF":9.3000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11520665/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13054-024-05117-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rezafungin is an echinocandin approved in the US and EU to treat candidaemia and/or invasive candidiasis. This post-hoc, pooled analysis of the Phase 2 STRIVE and Phase 3 ReSTORE trials assessed rezafungin versus caspofungin in patients with candidaemia and/or invasive candidiasis (IC) in the intensive care unit (ICU) at randomisation.
Methods: STRIVE and ReSTORE were randomised double-blind trials in adults with systemic signs and mycological confirmation of candidaemia and/or IC in blood or a normally sterile site ≤ 96 h before randomisation. Data were pooled for patients in the ICU at randomisation who received intravenous rezafungin (400 mg loading dose then 200 mg once weekly) or caspofungin (70 mg loading dose then 50 mg once daily) for ≤ 4 weeks. Outcomes were Day 30 all-cause mortality (primary outcome), Day 5 and 14 mycological eradication, time to negative blood culture, mortality attributable to candidaemia/invasive candidiasis, safety, and pharmacokinetics.
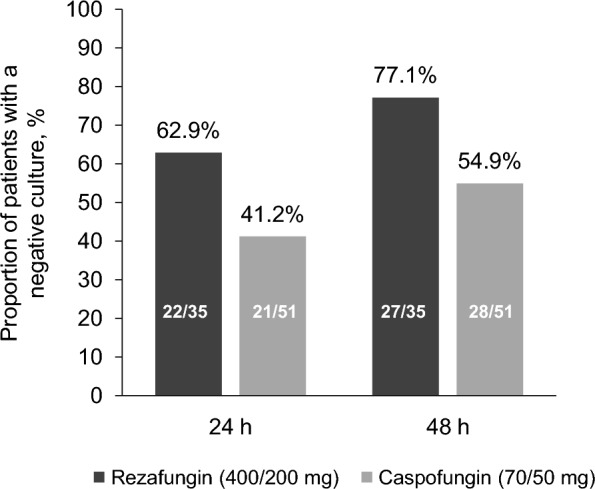
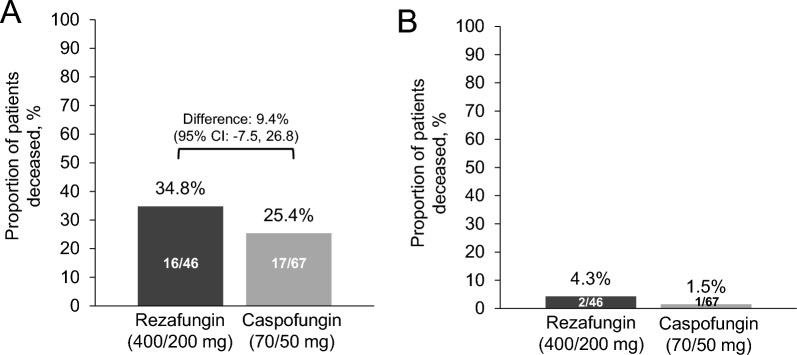
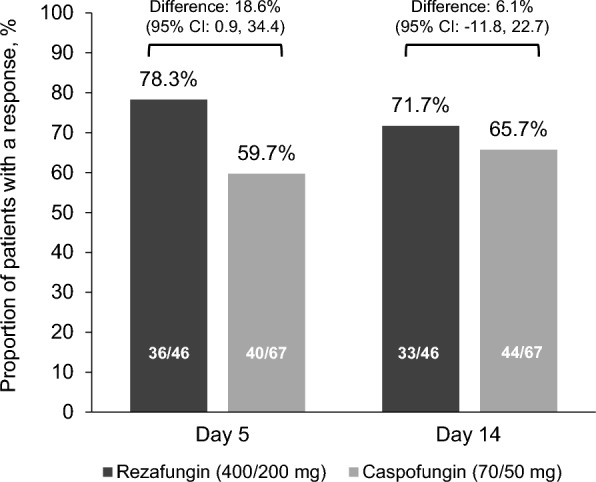
Results: Of 294 patients in STRIVE/ReSTORE, 113 were in the ICU at randomisation (rezafungin n = 46; caspofungin n = 67). At baseline, ~ 30% of patients in each group had impaired renal function and/or an Acute Physiologic Assessment and Chronic Health Evaluation II score ≥ 20. One patient (in the caspofungin group) was neutropenic at baseline. Day 30 all-cause mortality was 34.8% for rezafungin versus 25.4% for caspofungin. Day 5 and 14 mycological eradication was 78.3% and 71.7% for rezafungin versus 59.7% and 65.7% for caspofungin, respectively. Median time to negative blood culture was 18 (interquartile range, 12.6-43.0) versus 38 (interquartile range, 15.9-211.3) h for rezafungin versus caspofungin (stratified log-rank P = 0.001; nominal, not adjusted for multiplicity). Candidaemia/IC-attributable deaths occurred in two rezafungin patients versus one caspofungin patient. Safety profiles were similar between groups. Overall, 17.4% (rezafungin) versus 29.9% (caspofungin) of patients discontinued due to treatment-emergent adverse events. Rezafungin exposure following the initial 400-mg dose was comparable between patients in the ICU at randomisation (n = 50) and non-ICU patients (n = 117).
Conclusions: Rezafungin was well tolerated and efficacious in critically ill, mainly non-neutropenic patients with candidaemia and/or IC. This analysis provides additional insights into the efficacy and safety of rezafungin in the ICU population.
期刊介绍:
Critical Care is an esteemed international medical journal that undergoes a rigorous peer-review process to maintain its high quality standards. Its primary objective is to enhance the healthcare services offered to critically ill patients. To achieve this, the journal focuses on gathering, exchanging, disseminating, and endorsing evidence-based information that is highly relevant to intensivists. By doing so, Critical Care seeks to provide a thorough and inclusive examination of the intensive care field.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
