Giuseppe Pinto MD , Mauro Chiarito MD, PhD , Tania Puscas MD , Anne Bacher BSc , Erwan Donal MD, PhD , Patricia Reant MD, PhD , Gianluigi Condorelli MD, PhD , Albert Hagège MD, PhD , REMY working group of the French Society of Cardiology
{"title":"Comparative Influences of Beta blockers and Verapamil on Cardiac Outcomes in Hypertrophic Cardiomyopathy","authors":"Giuseppe Pinto MD , Mauro Chiarito MD, PhD , Tania Puscas MD , Anne Bacher BSc , Erwan Donal MD, PhD , Patricia Reant MD, PhD , Gianluigi Condorelli MD, PhD , Albert Hagège MD, PhD , REMY working group of the French Society of Cardiology","doi":"10.1016/j.amjcard.2024.10.029","DOIUrl":null,"url":null,"abstract":"<div><div>Guidelines recommend β blockers (BBs) as first-line therapy in symptomatic patients with hypertrophic cardiomyopathy (HCM) and nondihydropyridine calcium channel blockers, particularly, verapamil, as the second-line therapy, despite the absence of comparison trials between those 2 drugs. Because deleterious effects of verapamil have been reported in this setting, the present analysis aimed to evaluate the prognostic impact of BBs and verapamil in a cohort of patients with HCM. From a nationwide cohort of 1,434 patients with a diagnosis of HCM included in the French prospective observational REgistry of hypertrophic cardioMYopathy (REMY), we retrospectively analyzed patients with sarcomeric HCM included in the 3 largest centers and treated either with BBs or verapamil. Patients with a cardiac defibrillator or a pacemaker or who underwent a procedure of atrial fibrillation or septal ablation were excluded. The primary end point was the composite of cardiovascular death, hospitalization for heart failure, and hospitalization for atrial fibrillation. Of 600 patients with HCM, 544 (91%) were treated with BBs and 56 (9%) with verapamil. At inclusion, the 2 groups were comparable concerning the presence/amplitude of obstruction and sudden cardiac death risk factors. At up to 8 years of follow-up (median 3.9 years, interquartile range 2.1 to 5.8), no significant differences were observed in the primary end point (132 [24%] vs 10 [18%] under BBs or verapamil, respectively, hazard ratio 1.84, 95% confidence interval 0.94 to 3.63). In conclusion, in a real-world cohort of low-risk patients with HCM, verapamil therapy was not associated with a higher incidence of adverse events than β-blocker therapy.</div></div>","PeriodicalId":7705,"journal":{"name":"American Journal of Cardiology","volume":"235 ","pages":"Pages 9-15"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Cardiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0002914924007690","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
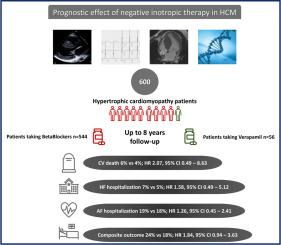
Guidelines recommend β blockers (BBs) as first-line therapy in symptomatic patients with hypertrophic cardiomyopathy (HCM) and nondihydropyridine calcium channel blockers, particularly, verapamil, as the second-line therapy, despite the absence of comparison trials between those 2 drugs. Because deleterious effects of verapamil have been reported in this setting, the present analysis aimed to evaluate the prognostic impact of BBs and verapamil in a cohort of patients with HCM. From a nationwide cohort of 1,434 patients with a diagnosis of HCM included in the French prospective observational REgistry of hypertrophic cardioMYopathy (REMY), we retrospectively analyzed patients with sarcomeric HCM included in the 3 largest centers and treated either with BBs or verapamil. Patients with a cardiac defibrillator or a pacemaker or who underwent a procedure of atrial fibrillation or septal ablation were excluded. The primary end point was the composite of cardiovascular death, hospitalization for heart failure, and hospitalization for atrial fibrillation. Of 600 patients with HCM, 544 (91%) were treated with BBs and 56 (9%) with verapamil. At inclusion, the 2 groups were comparable concerning the presence/amplitude of obstruction and sudden cardiac death risk factors. At up to 8 years of follow-up (median 3.9 years, interquartile range 2.1 to 5.8), no significant differences were observed in the primary end point (132 [24%] vs 10 [18%] under BBs or verapamil, respectively, hazard ratio 1.84, 95% confidence interval 0.94 to 3.63). In conclusion, in a real-world cohort of low-risk patients with HCM, verapamil therapy was not associated with a higher incidence of adverse events than β-blocker therapy.
期刊介绍:
Published 24 times a year, The American Journal of Cardiology® is an independent journal designed for cardiovascular disease specialists and internists with a subspecialty in cardiology throughout the world. AJC is an independent, scientific, peer-reviewed journal of original articles that focus on the practical, clinical approach to the diagnosis and treatment of cardiovascular disease. AJC has one of the fastest acceptance to publication times in Cardiology. Features report on systemic hypertension, methodology, drugs, pacing, arrhythmia, preventive cardiology, congestive heart failure, valvular heart disease, congenital heart disease, and cardiomyopathy. Also included are editorials, readers'' comments, and symposia.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
