Sandar Aye, Oskar Frisell, Henrik Zetterberg, Tobias Borgh Skillbäck, Silke Kern, Maria Eriksdotter, Emil Aho, Xin Xia, Bengt Winblad, Anders Wimo, Linus Jönsson
{"title":"Costs of Care in Relation to Alzheimer's Disease Severity in Sweden: A National Registry-Based Cohort Study.","authors":"Sandar Aye, Oskar Frisell, Henrik Zetterberg, Tobias Borgh Skillbäck, Silke Kern, Maria Eriksdotter, Emil Aho, Xin Xia, Bengt Winblad, Anders Wimo, Linus Jönsson","doi":"10.1007/s40273-024-01443-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The advancement of diagnostic and therapeutic interventions in early Alzheimer's disease (AD) has demanded the economic evaluation of such interventions. Resource utilization and cost estimates in early AD and, more specifically, the amyloid-positive population are still lacking. We aimed to provide cost estimates in AD in relation to disease severity and compare these with the control population. We also aimed to provide cost estimates for a subset of the AD population with both clinical diagnosis and amyloid-positive confirmation.</p><p><strong>Materials and methods: </strong>This was a retrospective longitudinal analysis of resource utilization using data from national registries. A cohort from the national Swedish registry for cognitive/dementia disorders (SveDem) includes all clinically diagnosed AD between 2013 and 2020. The study population included 31,951 people with AD and 63,902 age- and sex-matched controls (1:2). The population was followed until death, the end of December 2020, or 2 years from the last clinic visit. Direct medical and social costs were estimated from other national registries. Direct medical costs include costs for medications and inpatient and outpatient clinical visits. Direct social costs include costs for institutionalization, home care, short-term care, support for daytime activities, and housing support. Mean annual costs and 95% confidence intervals were obtained by bootstrapping, presented in 2021 Swedish Krona (SEK) (1 SEK = 0.117 USD, 1 SEK = 0.0985 EUR in 2021), and disaggregated by AD severity, cost component, sex, age group, and care setting.</p><p><strong>Results: </strong>Mean annual costs for individuals with clinically diagnosed AD were SEK 99,906, SEK 290,972, SEK 479,524, and SEK 795,617 in mild cognitive impairment (MCI), mild, moderate, and severe AD. The mean annual costs for the population with both clinical diagnosis and amyloid-positive AD confirmation (N = 5610) were SEK 57,625, SEK 179,153, SEK 333,095, and SEK 668,073 in MCI, mild, moderate, and severe AD, respectively. The mean annual costs were higher in institutionalized than non-institutionalized patients, females than males, and older than younger age groups. Inpatient and drug costs were similar in all AD severity stages, but outpatient costs decreased with AD severity. Costs for institutionalization, home care, support for daytime activities, and short-term care increased with AD severity, whereas the cost of housing support decreased with AD severity.</p><p><strong>Conclusions: </strong>This is the first study estimating annual costs in people with AD from MCI to severe AD, including those for the amyloid-positive population. The study provides cost estimates by AD severity, cost components, care settings, sex, and age groups, allowing health economic modelers to apply the costs based on different model structures and populations.</p>","PeriodicalId":19807,"journal":{"name":"PharmacoEconomics","volume":" ","pages":"153-169"},"PeriodicalIF":4.6000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11782292/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40273-024-01443-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The advancement of diagnostic and therapeutic interventions in early Alzheimer's disease (AD) has demanded the economic evaluation of such interventions. Resource utilization and cost estimates in early AD and, more specifically, the amyloid-positive population are still lacking. We aimed to provide cost estimates in AD in relation to disease severity and compare these with the control population. We also aimed to provide cost estimates for a subset of the AD population with both clinical diagnosis and amyloid-positive confirmation.
Materials and methods: This was a retrospective longitudinal analysis of resource utilization using data from national registries. A cohort from the national Swedish registry for cognitive/dementia disorders (SveDem) includes all clinically diagnosed AD between 2013 and 2020. The study population included 31,951 people with AD and 63,902 age- and sex-matched controls (1:2). The population was followed until death, the end of December 2020, or 2 years from the last clinic visit. Direct medical and social costs were estimated from other national registries. Direct medical costs include costs for medications and inpatient and outpatient clinical visits. Direct social costs include costs for institutionalization, home care, short-term care, support for daytime activities, and housing support. Mean annual costs and 95% confidence intervals were obtained by bootstrapping, presented in 2021 Swedish Krona (SEK) (1 SEK = 0.117 USD, 1 SEK = 0.0985 EUR in 2021), and disaggregated by AD severity, cost component, sex, age group, and care setting.
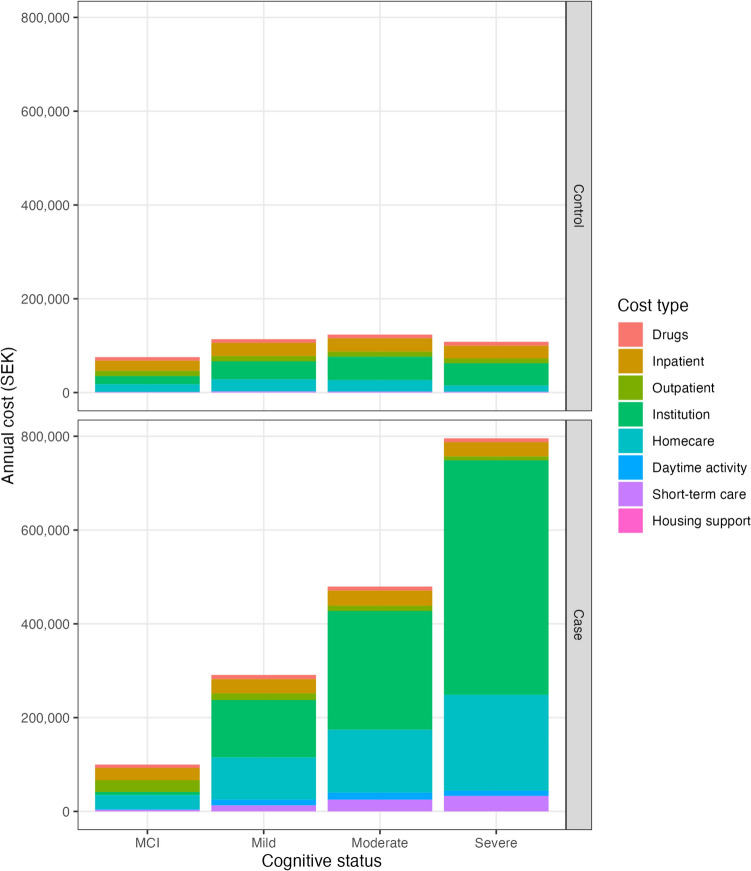
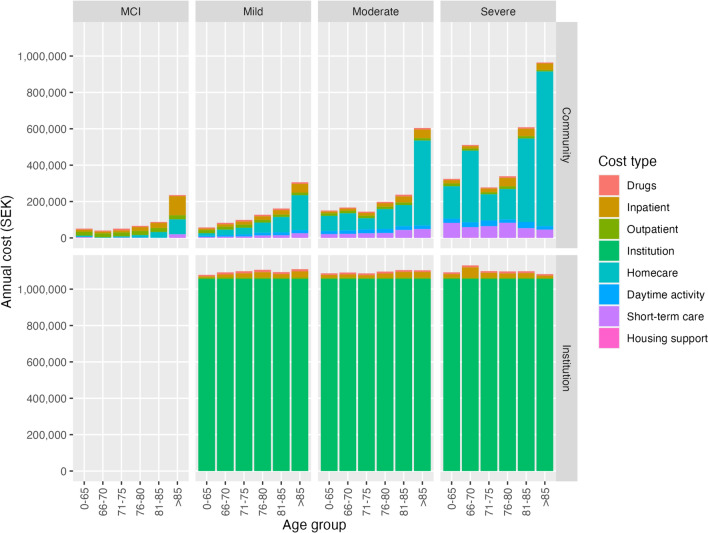
Results: Mean annual costs for individuals with clinically diagnosed AD were SEK 99,906, SEK 290,972, SEK 479,524, and SEK 795,617 in mild cognitive impairment (MCI), mild, moderate, and severe AD. The mean annual costs for the population with both clinical diagnosis and amyloid-positive AD confirmation (N = 5610) were SEK 57,625, SEK 179,153, SEK 333,095, and SEK 668,073 in MCI, mild, moderate, and severe AD, respectively. The mean annual costs were higher in institutionalized than non-institutionalized patients, females than males, and older than younger age groups. Inpatient and drug costs were similar in all AD severity stages, but outpatient costs decreased with AD severity. Costs for institutionalization, home care, support for daytime activities, and short-term care increased with AD severity, whereas the cost of housing support decreased with AD severity.
Conclusions: This is the first study estimating annual costs in people with AD from MCI to severe AD, including those for the amyloid-positive population. The study provides cost estimates by AD severity, cost components, care settings, sex, and age groups, allowing health economic modelers to apply the costs based on different model structures and populations.
期刊介绍:
PharmacoEconomics is the benchmark journal for peer-reviewed, authoritative and practical articles on the application of pharmacoeconomics and quality-of-life assessment to optimum drug therapy and health outcomes. An invaluable source of applied pharmacoeconomic original research and educational material for the healthcare decision maker.
PharmacoEconomics is dedicated to the clear communication of complex pharmacoeconomic issues related to patient care and drug utilization.
PharmacoEconomics offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by a Key Points summary, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
