Low Aortic Pulsatility Index and Pulmonary Artery Pulsatility Index Are Associated With Increased Mortality in Patients With Dilated Cardiomyopathy Awaiting Heart Transplantation.
{"title":"Low Aortic Pulsatility Index and Pulmonary Artery Pulsatility Index Are Associated With Increased Mortality in Patients With Dilated Cardiomyopathy Awaiting Heart Transplantation.","authors":"Yihang Wu, Yuhui Zhang, Jian Zhang","doi":"10.4070/kcj.2024.0192","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Patients with dilated cardiomyopathy (DCM) tend to be accompanied by biventricular impairment. We hypothesized that the combination of the aortic pulsatility index (API) and pulmonary artery pulsatility index (PAPI) could refine risk stratification in DCM.</p><p><strong>Methods: </strong>We studied 120 consecutive patients with advanced DCM who underwent right heart catheterization (RHC). The primary outcome was all-cause mortality within 1 year after RHC. We used the receiver operating characteristic curve to determine the optimal cut-off of API and PAPI to predict outcomes.</p><p><strong>Results: </strong>The optimal cut-offs of API (1.02) and PAPI (2.16) were used to classify patients into four groups. There were significant differences in left ventricular ejection fraction (LVEF) and tricuspid annular plane systolic excursion (TAPSE) among the four groups (both p<0.05). When delineating API by LVEF above or below the median (28%), the cumulative rate of survival in patients with API <1.02 was lower than that of those with API ≥1.02 in both higher and lower LVEF groups (both p<0.05). Similar trends were observed when delineating PAPI using TAPSE higher or lower than the cut-off (17 mm) (both p<0.05). The cumulative rate of survival in the API <1.02 and PAPI <2.16 group was lower than that in the API ≥1.02 and/or PAPI ≥2.16 (all p<0.05).</p><p><strong>Conclusions: </strong>API and PAPI could add additional prognostic value to LVEF and TAPSE, respectively. The combination of API and PAPI could provide a comprehensive assessment of biventricular function and refine risk stratification.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT02664818.</p>","PeriodicalId":17850,"journal":{"name":"Korean Circulation Journal","volume":" ","pages":"134-147"},"PeriodicalIF":3.1000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11875975/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Circulation Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4070/kcj.2024.0192","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
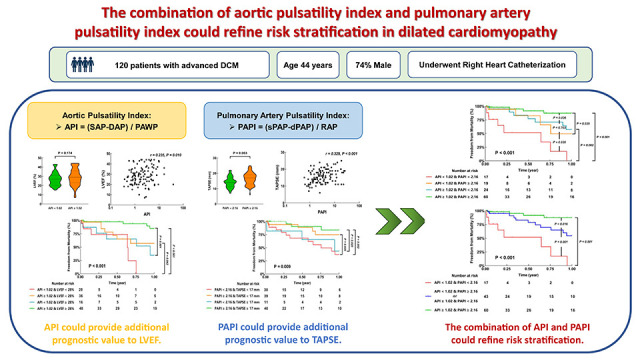
Background and objectives: Patients with dilated cardiomyopathy (DCM) tend to be accompanied by biventricular impairment. We hypothesized that the combination of the aortic pulsatility index (API) and pulmonary artery pulsatility index (PAPI) could refine risk stratification in DCM.
Methods: We studied 120 consecutive patients with advanced DCM who underwent right heart catheterization (RHC). The primary outcome was all-cause mortality within 1 year after RHC. We used the receiver operating characteristic curve to determine the optimal cut-off of API and PAPI to predict outcomes.
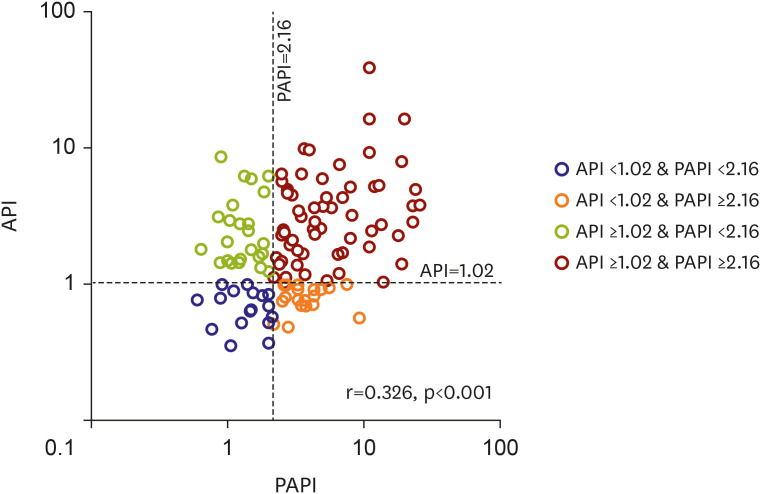
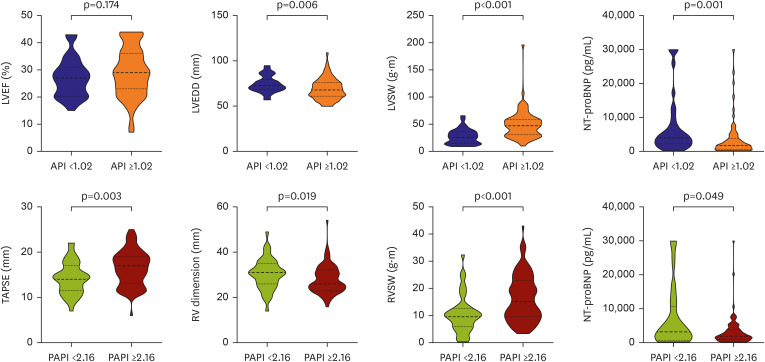
Results: The optimal cut-offs of API (1.02) and PAPI (2.16) were used to classify patients into four groups. There were significant differences in left ventricular ejection fraction (LVEF) and tricuspid annular plane systolic excursion (TAPSE) among the four groups (both p<0.05). When delineating API by LVEF above or below the median (28%), the cumulative rate of survival in patients with API <1.02 was lower than that of those with API ≥1.02 in both higher and lower LVEF groups (both p<0.05). Similar trends were observed when delineating PAPI using TAPSE higher or lower than the cut-off (17 mm) (both p<0.05). The cumulative rate of survival in the API <1.02 and PAPI <2.16 group was lower than that in the API ≥1.02 and/or PAPI ≥2.16 (all p<0.05).
Conclusions: API and PAPI could add additional prognostic value to LVEF and TAPSE, respectively. The combination of API and PAPI could provide a comprehensive assessment of biventricular function and refine risk stratification.
期刊介绍:
Korean Circulation Journal is the official journal of the Korean Society of Cardiology, the Korean Pediatric Heart Society, the Korean Society of Interventional Cardiology, and the Korean Society of Heart Failure. Abbreviated title is ''Korean Circ J''.
Korean Circulation Journal, established in 1971, is a professional, peer-reviewed journal covering all aspects of cardiovascular medicine, including original articles of basic research and clinical findings, review articles, editorials, images in cardiovascular medicine, and letters to the editor. Korean Circulation Journal is published monthly in English and publishes scientific and state-of-the-art clinical articles aimed at improving human health in general and contributing to the treatment and prevention of cardiovascular diseases in particular.
The journal is published on the official website (https://e-kcj.org). It is indexed in PubMed, PubMed Central, Science Citation Index Expanded (SCIE, Web of Science), Scopus, EMBASE, Chemical Abstracts Service (CAS), Google Scholar, KoreaMed, KoreaMed Synapse and KoMCI, and easily available to wide international researchers



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
