Pietro Scilipoti , Marco Moschini , Mario de Angelis , Mattia Longoni , Luca Afferi , Chiara Lonati , Paolo Zaurito , Renate Pichler , Andrea Necchi , Francesco Montorsi , Alberto Briganti , Andrea Mari , Wojciech Krajewski , Ekaterina Laukthina , Benjamin Pradere , Francesco Del Giudice , Laura Mertens , Andrea Gallioli , Francesco Soria , Paolo Gontero , Roberto Carando
{"title":"Risk of Metachronous Upper Tract Urothelial Carcinoma After Ureteral Stenting in Patients With Bladder Cancer","authors":"Pietro Scilipoti , Marco Moschini , Mario de Angelis , Mattia Longoni , Luca Afferi , Chiara Lonati , Paolo Zaurito , Renate Pichler , Andrea Necchi , Francesco Montorsi , Alberto Briganti , Andrea Mari , Wojciech Krajewski , Ekaterina Laukthina , Benjamin Pradere , Francesco Del Giudice , Laura Mertens , Andrea Gallioli , Francesco Soria , Paolo Gontero , Roberto Carando","doi":"10.1016/j.clgc.2024.102241","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Sparse data exist on the impact of upper urinary tract (UUT) decompression on the risk of UUT recurrence in patients with bladder cancer (BCa). This study aims to evaluate whether Double J stenting (DJS) can increase the risk of UUT recurrence compared to percutaneous nephrostomy (PCN) placement.</div></div><div><h3>Materials and methods</h3><div>We retrospectively analyzed data from 1550 patients with cTa-T3NanyM0 BCa who underwent radical cystectomy (RC) between at 12 tertiary care centers (1990-2020). Patients with complete follow-up, no prior history of UUT cancer, and who required UUT decompression for preoperative hydronephrosis were selected. Hydronephrosis grade was defined according to established scoring systems. UUT recurrence was diagnosed through imaging, urinary cytology, and confirmed by selective cytology and ureteroscopy when possible. Propensity scores were computed to determine overlap weights and balance groups. Kaplan–Meier analyses estimated UUT recurrence-free survival (RFS), cancer-specific (CSS), and overall survival (OS) before and after weighting. Cox regression analyses before and after weighting were fitted to predict UUT recurrence.</div></div><div><h3>Results</h3><div>Of 524 included patients, 132 (25%) and 392 (75%) patients were managed with DJS and PCN placement, respectively. Patients who received PCN had higher grade (≥ 3) of obstruction (34% vs. 14%) and pT3-4 tumors (70% vs. 36%) than patients with DJS. During a median follow-up of 19 months, 2-years UUT-RFS did not differ between groups (95% for PCN vs 92% for DJS, weighted HR 1.41, 95% CI, 0.55-3.59). There was no difference in 2-years weighted CSS (74% vs. 74%) and OS (67% vs 69%). Main limitations were the short follow-up and inclusion of patients uniquely undergoing RC.</div></div><div><h3>Conclusions</h3><div>These results suggest that ureteral DJS does not increase the risk of developing UUT recurrence in BCa patients with hydronephrosis requiring UUT decompression. However, UUT recurrence was rare, and associations were weak, with findings susceptible to bias. Randomized trials are needed to validate these results.</div></div>","PeriodicalId":10380,"journal":{"name":"Clinical genitourinary cancer","volume":"22 6","pages":"Article 102241"},"PeriodicalIF":2.7000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical genitourinary cancer","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1558767324002118","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/17 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
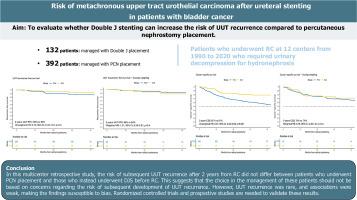
Sparse data exist on the impact of upper urinary tract (UUT) decompression on the risk of UUT recurrence in patients with bladder cancer (BCa). This study aims to evaluate whether Double J stenting (DJS) can increase the risk of UUT recurrence compared to percutaneous nephrostomy (PCN) placement.
Materials and methods
We retrospectively analyzed data from 1550 patients with cTa-T3NanyM0 BCa who underwent radical cystectomy (RC) between at 12 tertiary care centers (1990-2020). Patients with complete follow-up, no prior history of UUT cancer, and who required UUT decompression for preoperative hydronephrosis were selected. Hydronephrosis grade was defined according to established scoring systems. UUT recurrence was diagnosed through imaging, urinary cytology, and confirmed by selective cytology and ureteroscopy when possible. Propensity scores were computed to determine overlap weights and balance groups. Kaplan–Meier analyses estimated UUT recurrence-free survival (RFS), cancer-specific (CSS), and overall survival (OS) before and after weighting. Cox regression analyses before and after weighting were fitted to predict UUT recurrence.
Results
Of 524 included patients, 132 (25%) and 392 (75%) patients were managed with DJS and PCN placement, respectively. Patients who received PCN had higher grade (≥ 3) of obstruction (34% vs. 14%) and pT3-4 tumors (70% vs. 36%) than patients with DJS. During a median follow-up of 19 months, 2-years UUT-RFS did not differ between groups (95% for PCN vs 92% for DJS, weighted HR 1.41, 95% CI, 0.55-3.59). There was no difference in 2-years weighted CSS (74% vs. 74%) and OS (67% vs 69%). Main limitations were the short follow-up and inclusion of patients uniquely undergoing RC.
Conclusions
These results suggest that ureteral DJS does not increase the risk of developing UUT recurrence in BCa patients with hydronephrosis requiring UUT decompression. However, UUT recurrence was rare, and associations were weak, with findings susceptible to bias. Randomized trials are needed to validate these results.
期刊介绍:
Clinical Genitourinary Cancer is a peer-reviewed journal that publishes original articles describing various aspects of clinical and translational research in genitourinary cancers. Clinical Genitourinary Cancer is devoted to articles on detection, diagnosis, prevention, and treatment of genitourinary cancers. The main emphasis is on recent scientific developments in all areas related to genitourinary malignancies. Specific areas of interest include clinical research and mechanistic approaches; drug sensitivity and resistance; gene and antisense therapy; pathology, markers, and prognostic indicators; chemoprevention strategies; multimodality therapy; and integration of various approaches.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
