Caitlin E Martinez, Brooke T Nezami, Elizabeth Mayer-Davis, Erik A Willis, Amy A Gorin, Deborah F Tate
{"title":"Results of a pilot sequential multiple assignment randomized trial using counseling to augment a digital weight loss program.","authors":"Caitlin E Martinez, Brooke T Nezami, Elizabeth Mayer-Davis, Erik A Willis, Amy A Gorin, Deborah F Tate","doi":"10.1002/osp4.70018","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Adaptive interventions may improve the potency and scalability of behavioral weight loss interventions, but the treatments-or treatment combinations-that should be offered are unknown. A two-stage pilot sequential multiple assignment randomized trial was used to test the timing and dose of human support added to a core digital weight loss program.</p><p><strong>Methods: </strong>In stage 1, 99 adults with overweight/obesity were randomized at baseline to a kick-off with or without additional human support. In stage 2, \"early non-responders\" who had not achieved a 2% weight loss were re-randomized after 4 weeks to either biweekly counseling (120 min over 8 weeks) or a one-time check-in (30 min) with a dietitian. \"Early responders\" continued with the mHealth program alone. Feasibility and acceptability were assessed against pre-specified criteria. Preliminary outcomes (weight loss, self-monitoring and behavioral goal adherence) were explored.</p><p><strong>Results: </strong>The study met all feasibility and acceptability criteria. The rate of early response was 52.5%. Mean (SE) 3-month percent weight losses were significantly greater in early responders (-6.63% (0.72)) than non-responders (-1.70% (0.43), <i>p</i> < 0.001). Outcomes were similar by first- and second-line treatment though more counseling (27.3%) than check-in (12.5%) participants achieved a 5% weight loss.</p><p><strong>Conclusions: </strong>Identifying early responders may help optimize weight loss interventions, but more research is needed on rescue treatments for early non-responders.</p><p><strong>Trial registration: </strong>ClinicalTrial.gov, NCT05929469.</p>","PeriodicalId":19448,"journal":{"name":"Obesity Science & Practice","volume":"10 6","pages":"e70018"},"PeriodicalIF":1.9000,"publicationDate":"2024-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11541063/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Science & Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/osp4.70018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
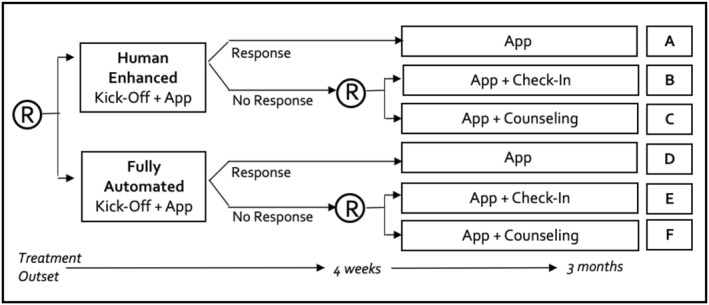
Objective: Adaptive interventions may improve the potency and scalability of behavioral weight loss interventions, but the treatments-or treatment combinations-that should be offered are unknown. A two-stage pilot sequential multiple assignment randomized trial was used to test the timing and dose of human support added to a core digital weight loss program.
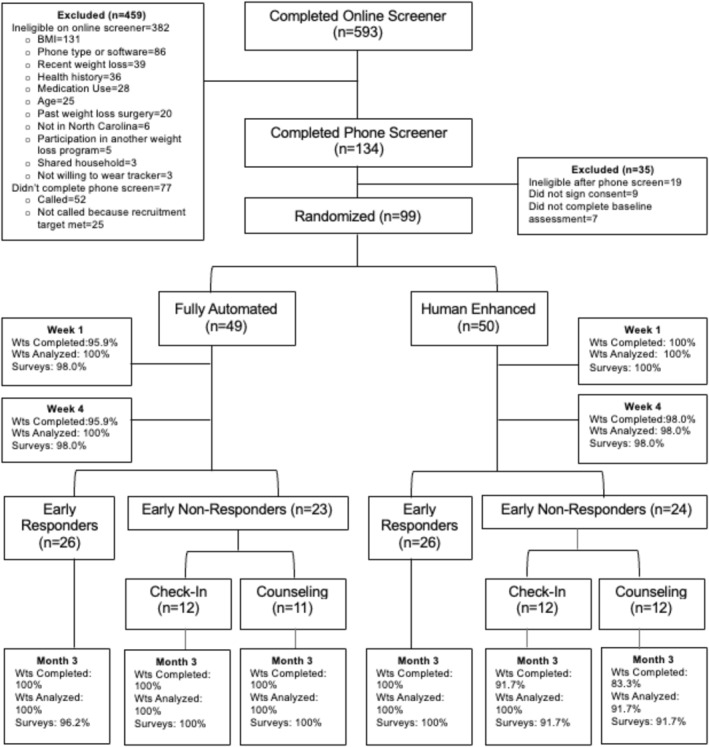
Methods: In stage 1, 99 adults with overweight/obesity were randomized at baseline to a kick-off with or without additional human support. In stage 2, "early non-responders" who had not achieved a 2% weight loss were re-randomized after 4 weeks to either biweekly counseling (120 min over 8 weeks) or a one-time check-in (30 min) with a dietitian. "Early responders" continued with the mHealth program alone. Feasibility and acceptability were assessed against pre-specified criteria. Preliminary outcomes (weight loss, self-monitoring and behavioral goal adherence) were explored.
Results: The study met all feasibility and acceptability criteria. The rate of early response was 52.5%. Mean (SE) 3-month percent weight losses were significantly greater in early responders (-6.63% (0.72)) than non-responders (-1.70% (0.43), p < 0.001). Outcomes were similar by first- and second-line treatment though more counseling (27.3%) than check-in (12.5%) participants achieved a 5% weight loss.
Conclusions: Identifying early responders may help optimize weight loss interventions, but more research is needed on rescue treatments for early non-responders.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
