Real-life effectiveness on overall survival of continued immune checkpoint inhibition following progression in advanced melanoma: estimation from the Melbase cohort.
Camille Macaire, Wendy Lefevre, Sophie Dalac, Henri Montaudié, Delphine Legoupil, Olivier Dereure, Caroline Dutriaux, Marie Thérèse Leccia, François Aubin, Jean Jacques Grob, Philippe Saiag, Julie De Quatrebarbes, Eve Maubec, Thierry Lesimple, Florence Granel-Brocard, Laurent Mortier, Stéphane Dalle, Céleste Lebbé, Chloé Prod'homme
{"title":"Real-life effectiveness on overall survival of continued immune checkpoint inhibition following progression in advanced melanoma: estimation from the Melbase cohort.","authors":"Camille Macaire, Wendy Lefevre, Sophie Dalac, Henri Montaudié, Delphine Legoupil, Olivier Dereure, Caroline Dutriaux, Marie Thérèse Leccia, François Aubin, Jean Jacques Grob, Philippe Saiag, Julie De Quatrebarbes, Eve Maubec, Thierry Lesimple, Florence Granel-Brocard, Laurent Mortier, Stéphane Dalle, Céleste Lebbé, Chloé Prod'homme","doi":"10.1097/CMR.0000000000000973","DOIUrl":null,"url":null,"abstract":"<p><p>The link between palliative care and oncology must continue to develop, taking into account advances in treatment.Immune checkpoint inhibition (ICI) for metastatic melanoma is associated with different types of response, making it difficult to assess the benefits to the patient. Some clinical trials suggest a survival advantage of ICI even in the absence of an objective radiographic response. The aim of this study is to assess the impact of continuing ICI after progression of the disease on the overall survival (OS) in a cohort of final-line metastatic melanoma patients. Clinical data from 120 patients with metastatic melanoma were collected via Melbase, a French multicentric biobank, prospectively enrolling unresectable melanoma. Two groups were defined: patients continuing final-line ICI at progression (treated) and patients stopping ICI at progression (controls). The primary end-point is the OS from progression. Propensity score weighting was used to correct for indication bias. From the 120 patients, 72 (60%) continued ICI. Median OS from progression was 4.2 months [95% confidence interval (CI) 2.6-6.27] in the treated group and median OS was 1.3 months (95% CI 0.95-1.74) in the control group ( P < 0.0001). The calculated hazard ratio was 0.20 (0.13-0.33). Continued ICI was discovered to have an association with a higher rate of hospitalization at the end of life; more treatments received in the last 15 days of life and less utilization of specialist palliative care. This study discovered that patients with metastatic melanoma show a significant decrease in the instantaneous probability of mortality when they continue with finale-line ICI after progression.</p>","PeriodicalId":18550,"journal":{"name":"Melanoma Research","volume":" ","pages":"50-59"},"PeriodicalIF":1.9000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11670915/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Melanoma Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/CMR.0000000000000973","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
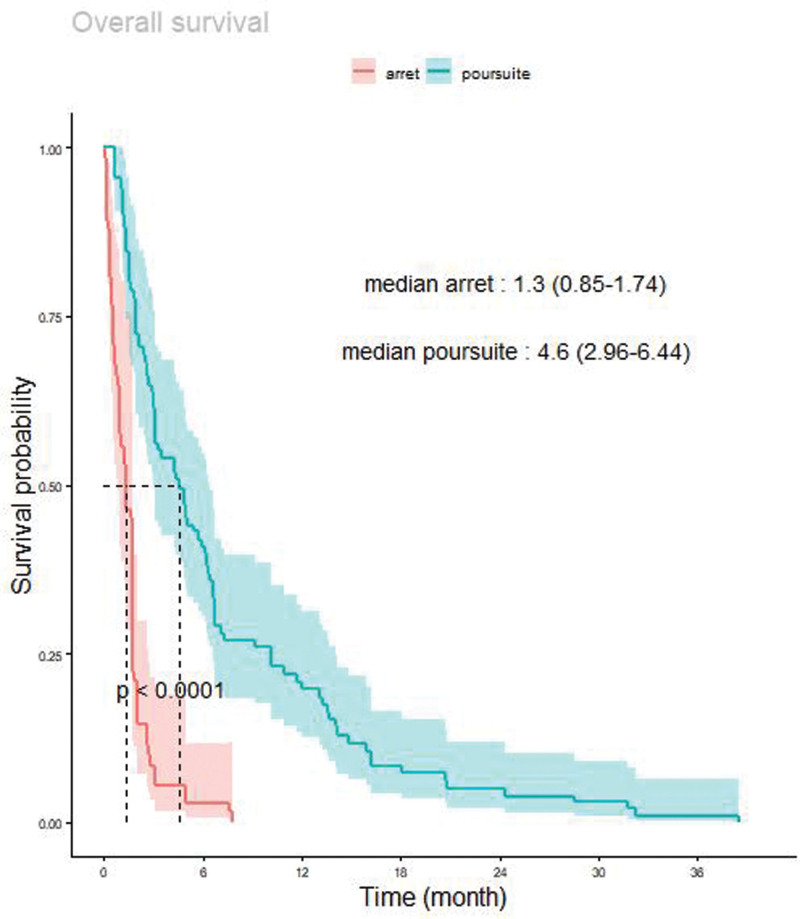
The link between palliative care and oncology must continue to develop, taking into account advances in treatment.Immune checkpoint inhibition (ICI) for metastatic melanoma is associated with different types of response, making it difficult to assess the benefits to the patient. Some clinical trials suggest a survival advantage of ICI even in the absence of an objective radiographic response. The aim of this study is to assess the impact of continuing ICI after progression of the disease on the overall survival (OS) in a cohort of final-line metastatic melanoma patients. Clinical data from 120 patients with metastatic melanoma were collected via Melbase, a French multicentric biobank, prospectively enrolling unresectable melanoma. Two groups were defined: patients continuing final-line ICI at progression (treated) and patients stopping ICI at progression (controls). The primary end-point is the OS from progression. Propensity score weighting was used to correct for indication bias. From the 120 patients, 72 (60%) continued ICI. Median OS from progression was 4.2 months [95% confidence interval (CI) 2.6-6.27] in the treated group and median OS was 1.3 months (95% CI 0.95-1.74) in the control group ( P < 0.0001). The calculated hazard ratio was 0.20 (0.13-0.33). Continued ICI was discovered to have an association with a higher rate of hospitalization at the end of life; more treatments received in the last 15 days of life and less utilization of specialist palliative care. This study discovered that patients with metastatic melanoma show a significant decrease in the instantaneous probability of mortality when they continue with finale-line ICI after progression.
期刊介绍:
Melanoma Research is a well established international forum for the dissemination of new findings relating to melanoma. The aim of the Journal is to promote the level of informational exchange between those engaged in the field. Melanoma Research aims to encourage an informed and balanced view of experimental and clinical research and extend and stimulate communication and exchange of knowledge between investigators with differing areas of expertise. This will foster the development of translational research. The reporting of new clinical results and the effect and toxicity of new therapeutic agents and immunotherapy will be given emphasis by rapid publication of Short Communications. Thus, Melanoma Research seeks to present a coherent and up-to-date account of all aspects of investigations pertinent to melanoma. Consequently the scope of the Journal is broad, embracing the entire range of studies from fundamental and applied research in such subject areas as genetics, molecular biology, biochemistry, cell biology, photobiology, pathology, immunology, and advances in clinical oncology influencing the prevention, diagnosis and treatment of melanoma.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
