{"title":"Recurrent peroneal tendon dislocation-the current concept of management.","authors":"Akinobu Nishimura, Yuki Fujikawa, Yoshiyuki Senga, Shigeto Nakazora, Chihiro Konno, Akihiro Sudo","doi":"10.21037/aoj-24-10","DOIUrl":null,"url":null,"abstract":"<p><p>The peroneus muscles, consisting of the peroneus longus (PL) and peroneus brevis (PB) tendons, are vulnerable to injury at anatomically specific sites or within tendon sheaths. Peroneal tendon dislocation (PTD) is often misdiagnosed as a lateral ankle sprain as it occurs at a lower frequency than a lateral ankle sprain. Anatomical variations in the retromalleolar groove, soft tissue overstuffing, and presence of accessory peroneal muscles contribute to the etiology of PTD. PTD has been classified into four types based on injury patterns involving the superior peroneal retinaculum (SPR) and fibrocartilaginous ridge. Diagnosis involves recognizing tender points and using imaging including magnetic resonance imaging (MRI) and ultrasonography. Conservative treatments, including below-knee plaster casts, have varying success rates, and some patients progress to recurrent PTD (RPTD), prompting consideration of surgical interventions. Diagnosis is easy in patients with RPTD who can reproduce the dislocation by themselves; however, in many cases, this is not possible. In such cases, ultrasonography after intrasheath injection is effective in confirming the presence of a pseudo-pouch. RPTD can be diagnosed if a pseudo-pouch is identified during ultrasonography. Surgical approaches such as osteotomy, soft tissue procedures, and groove deepening techniques are used to stabilize the peroneal tendons. Soft tissue procedures, especially SPR reattachment, have emerged as a preferred option, demonstrating outcomes comparable to those of osteotomy, with fewer complications. Intrasheath subluxation, a unique PTD subtype, is diagnosed using ultrasonography. In this type of subluxation, no damage to the SPR is observed, and the positions of the PL and PB tendons are interchanged. Surgical intervention may involve excision of the synovium and SPR repair. In cases of PTD complicated by a longitudinal rupture of the PB tendon, suturing of the torn area or tubularization of the remaining tendon for partial resection of the degenerated tendon can be performed. The purpose of this article is to describe the methods for diagnoses and management of PTD.</p>","PeriodicalId":44459,"journal":{"name":"Annals of Joint","volume":"9 ","pages":"40"},"PeriodicalIF":0.9000,"publicationDate":"2024-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558277/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Joint","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/aoj-24-10","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
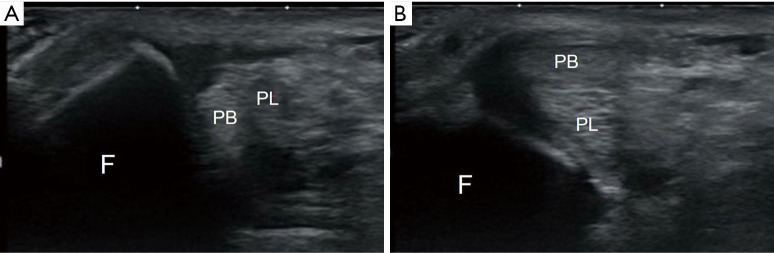
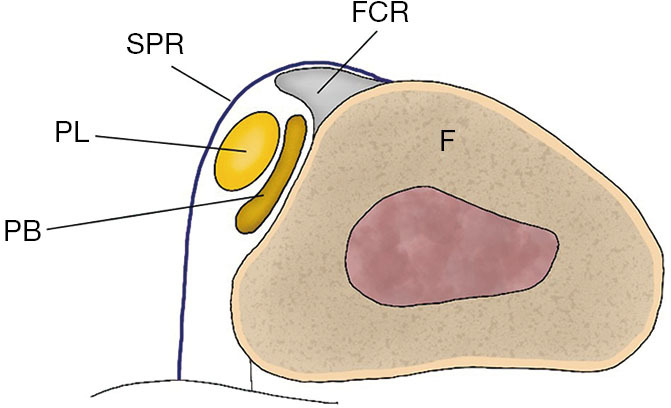
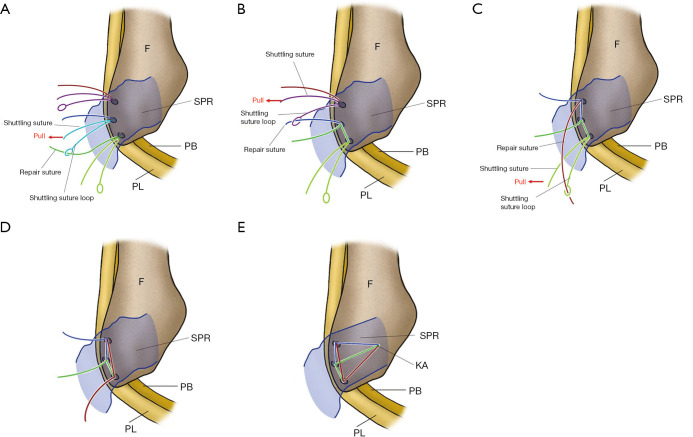
The peroneus muscles, consisting of the peroneus longus (PL) and peroneus brevis (PB) tendons, are vulnerable to injury at anatomically specific sites or within tendon sheaths. Peroneal tendon dislocation (PTD) is often misdiagnosed as a lateral ankle sprain as it occurs at a lower frequency than a lateral ankle sprain. Anatomical variations in the retromalleolar groove, soft tissue overstuffing, and presence of accessory peroneal muscles contribute to the etiology of PTD. PTD has been classified into four types based on injury patterns involving the superior peroneal retinaculum (SPR) and fibrocartilaginous ridge. Diagnosis involves recognizing tender points and using imaging including magnetic resonance imaging (MRI) and ultrasonography. Conservative treatments, including below-knee plaster casts, have varying success rates, and some patients progress to recurrent PTD (RPTD), prompting consideration of surgical interventions. Diagnosis is easy in patients with RPTD who can reproduce the dislocation by themselves; however, in many cases, this is not possible. In such cases, ultrasonography after intrasheath injection is effective in confirming the presence of a pseudo-pouch. RPTD can be diagnosed if a pseudo-pouch is identified during ultrasonography. Surgical approaches such as osteotomy, soft tissue procedures, and groove deepening techniques are used to stabilize the peroneal tendons. Soft tissue procedures, especially SPR reattachment, have emerged as a preferred option, demonstrating outcomes comparable to those of osteotomy, with fewer complications. Intrasheath subluxation, a unique PTD subtype, is diagnosed using ultrasonography. In this type of subluxation, no damage to the SPR is observed, and the positions of the PL and PB tendons are interchanged. Surgical intervention may involve excision of the synovium and SPR repair. In cases of PTD complicated by a longitudinal rupture of the PB tendon, suturing of the torn area or tubularization of the remaining tendon for partial resection of the degenerated tendon can be performed. The purpose of this article is to describe the methods for diagnoses and management of PTD.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
