
The transesophageal echocardiogram (TEE) is the standard imaging modality for confirming the presence or absence of patent foramen ovale. PFO is a flap valve depending on the pressure change between the left and right atrium, which can help determine whether to open. 3D-TEE was shown to optimize the visualization of PFO. There is a causal association between PFO and unexplained stroke. It seems that 3D-TEE can present a high-risk PFO morphological feature, which seems to show more than just being easier to open.
In total, 134 consecutive patients with cryptogenic stroke or migraine who had suspected PFO and underwent c-TCD, TTE, and c-TEE were included in this study. TEE confirmed the PFO. The right-to-left shunt (RLS) grade of PFO at rest and abdominal compression Valsalva maneuver was detected by c-TEE.
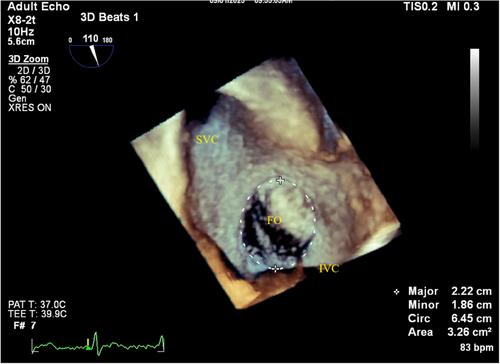
The long diameter of FO (1.74 ± 0.3 vs. 1.60 ± 0.4, p = 0.039), the short diameter of FO (1.12 ± 0.3 vs. 1.00 ± 0.3, p = 0.036), perimeter of FO (4.62 ± 0.7 vs. 4.22 ± 1.0, p = 0.026), and area (1.80 ± 0.8 vs. 1.35 ± 0.8, p = 0.05) of the FO were significantly larger in the larger RLS group. In group of CS, a larger proportion of Eustachian valve or a Chiari's network (14.3% vs. 3.5%, p = 0.036), a larger proportion of in the left funnelform (55.1% vs. 16.3%, p < 0.001), a longer length of the PFO tunnel (13.4 ± 4.4 vs. 7.8 ± 2.5, p < 0.001), a lower IVC-PFO angle (16.4 ± 3.4 vs. 20.3 ± 7.7, p = 0.001), a higher proportion of LA multiple exits of the tunnel (46.9% vs. 14.3%, p < 0.001). Multivariate regression analysis showed that male gender (HR: 4.026, 95% CI: 0.883–18.361, p = 0.072), age (HR: 1.076, 95% CI: 1.002–1.155, p = 0.045), the left funnelform (HR: 7.299, 95% CI: 1.585–33.618, p = 0.011), a longer length of the PFO tunnel (HR: 1.843, 95% CI: 1.404–2.418, p < 0.001) and multiple exits of the tunnel of LA (HR: 8.544, 95% CI: 1.595–45.754, p = 0.012) increased the risk of cerebral infarction. The cut-off value calculated by ROC for the diagnosis of high-risk PFO was that the length of the PFO tunnel was 12 mm and the left funnelform combined with multiple exits of the left atrial (sensitivity was 92%, specificity was 90%). The area under the curve of the combined index versus PoPE score (0.932 vs. 0.736) relative to the RoPE score was statistically significant.
TEE has shown outstanding advantages in displaying the specific morphological characteristics of PFO. The left funnelform, a longer length of the PFO tunnel, and multiple exits of the tunnel of LA are associated with an increasing risk of CS in anatomical PFO respect.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
