Ricardo Antônio Correia Lima, Annika Reintam Blaser, Júlia Falconiere Paredes Ramalho, Barbara Cristina de Almeida Campos Lacerda, Gabriela Sadigurschi, Paula Fonseca Aarestrup, Rafael Aguilar Sales, João Mansur Filho, Roberto Muniz Ferreira
{"title":"Prognostic significance of gastrointestinal dysfunction in critically ill patients with COVID-19.","authors":"Ricardo Antônio Correia Lima, Annika Reintam Blaser, Júlia Falconiere Paredes Ramalho, Barbara Cristina de Almeida Campos Lacerda, Gabriela Sadigurschi, Paula Fonseca Aarestrup, Rafael Aguilar Sales, João Mansur Filho, Roberto Muniz Ferreira","doi":"10.62675/2965-2774.20240020-en","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To analyze in-hospital and 1-year morbidity and mortality associated with acute gastrointestinal dysfunction in critically ill patients with COVID-19 via a prespecified scoring system.</p><p><strong>Methods: </strong>Between March and July 2020, consecutive hospitalized patients with COVID-19 from a single institution were retrospectively analyzed by medical chart review. Only those who remained in the intensive care unit for more than 24 hours were included. Gastrointestinal dysfunction was assessed according to a predefined 5-point progressive gastrointestinal injury scoring system, considering the first 7 days of hospitalization. Laboratory data, comorbidities, the need for mechanical ventilation, the duration of intensive care unit stay, and subsequent in-hospital and 1-year mortality rates were also recorded.</p><p><strong>Results: </strong>Among 230 patients who were screened, 215 were included in the analysis. The median age was 68 years (54 - 82), and 57.7% were male. The total gastrointestinal dysfunction scores were 0 (79.1%), I (15.3%), II (4.7%), III (0.9%), and IV (0%). Any manifestation of gastrointestinal dysfunction was present in 20.9% of all patients and was associated with longer lengths of stay (20 days [11 - 33] versus 7 days [4 - 16]; p < 0.001] and higher C-reactive protein levels on admission (12.8mg/mL [6.4 - 18.4] versus 5.7mg/mL [3.2 - 13.4]; p < 0.001). The gastrointestinal dysfunction score was significantly associated with mortality (OR 2.8; 95%CI 1.7 - 4.8; p < 0.001) and the need for mechanical ventilation (OR 2.8; 95%CI 1.7 - 4.6; p < 0.001). Both in-hospital and 1-year death rates progressively increased as gastrointestinal dysfunction scores increased.</p><p><strong>Conclusion: </strong>In the current series of intensive care unit patients with COVID-19, gastrointestinal dysfunction severity, as defined by a prespecified scoring system, was predictive of adverse in-hospital and 1-year outcomes.</p>","PeriodicalId":72721,"journal":{"name":"Critical care science","volume":"36 ","pages":"e20240020en"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11554297/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.62675/2965-2774.20240020-en","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To analyze in-hospital and 1-year morbidity and mortality associated with acute gastrointestinal dysfunction in critically ill patients with COVID-19 via a prespecified scoring system.
Methods: Between March and July 2020, consecutive hospitalized patients with COVID-19 from a single institution were retrospectively analyzed by medical chart review. Only those who remained in the intensive care unit for more than 24 hours were included. Gastrointestinal dysfunction was assessed according to a predefined 5-point progressive gastrointestinal injury scoring system, considering the first 7 days of hospitalization. Laboratory data, comorbidities, the need for mechanical ventilation, the duration of intensive care unit stay, and subsequent in-hospital and 1-year mortality rates were also recorded.
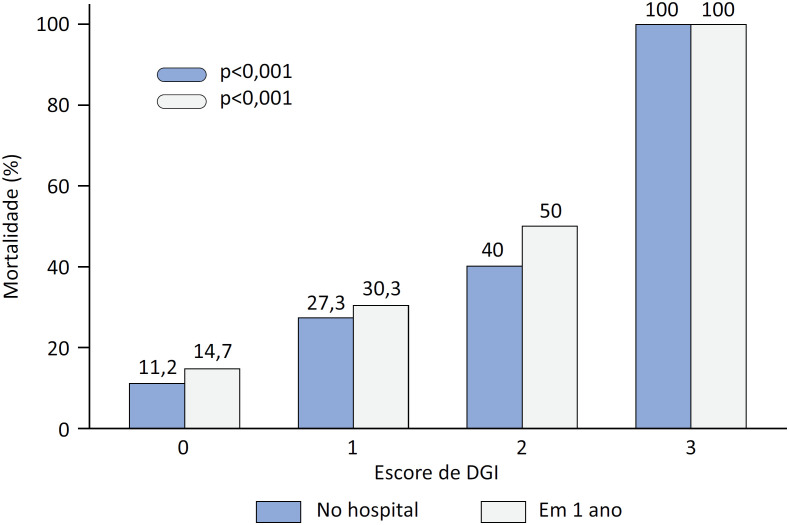
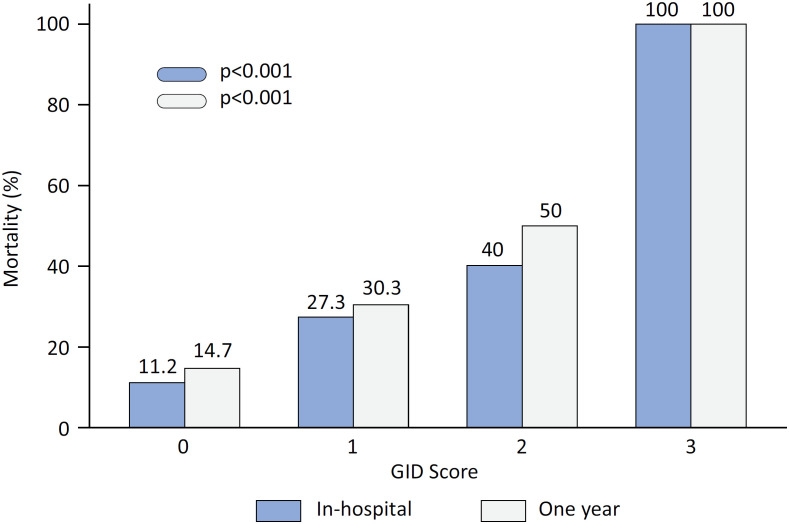
Results: Among 230 patients who were screened, 215 were included in the analysis. The median age was 68 years (54 - 82), and 57.7% were male. The total gastrointestinal dysfunction scores were 0 (79.1%), I (15.3%), II (4.7%), III (0.9%), and IV (0%). Any manifestation of gastrointestinal dysfunction was present in 20.9% of all patients and was associated with longer lengths of stay (20 days [11 - 33] versus 7 days [4 - 16]; p < 0.001] and higher C-reactive protein levels on admission (12.8mg/mL [6.4 - 18.4] versus 5.7mg/mL [3.2 - 13.4]; p < 0.001). The gastrointestinal dysfunction score was significantly associated with mortality (OR 2.8; 95%CI 1.7 - 4.8; p < 0.001) and the need for mechanical ventilation (OR 2.8; 95%CI 1.7 - 4.6; p < 0.001). Both in-hospital and 1-year death rates progressively increased as gastrointestinal dysfunction scores increased.
Conclusion: In the current series of intensive care unit patients with COVID-19, gastrointestinal dysfunction severity, as defined by a prespecified scoring system, was predictive of adverse in-hospital and 1-year outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
