Association of Sickle Cell Disease, Malaria and HIV in Multi Drug Resistant Invasive Non-typhoidal Salmonella Isolated from Outpatient and Hospitalised Children Below 16 Years in Informal Settlements in Nairobi County, Kenya.
Susan Mutile Kavai, Cecilia Mbae, Celestine Wairimu, Ronald Ngetich, Zillah Wakio, Robert Onsaŕe, Samuel Kariuki
{"title":"Association of Sickle Cell Disease, Malaria and HIV in Multi Drug Resistant Invasive Non-typhoidal <i>Salmonella</i> Isolated from Outpatient and Hospitalised Children Below 16 Years in Informal Settlements in Nairobi County, Kenya.","authors":"Susan Mutile Kavai, Cecilia Mbae, Celestine Wairimu, Ronald Ngetich, Zillah Wakio, Robert Onsaŕe, Samuel Kariuki","doi":"10.24248/easci.v6i1.92","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Invasive non-typhoidal <i>Salmonella</i> (iNTS) disease continues to be a major public health problem, especially in sub-Saharan Africa (SSA), where incidence rates are 227 cases [range 152-341] per 100,000 populations. Populations at risk of iNTS include adults with human immunodeficiency virus (HIV) infection, malnourished children, and those with recent malaria or sickle-cell anaemia (SCA). In Kenya, iNTS disease is particularly a major challenge in poor informal settlements, with infants and young children less than 5 years of age being the most affected. Our study aimed to investigate the association between sickle cell disease, malaria, and HIV in multi-drug-resistant invasive non-typhoidal <i>Salmonella</i> from outpatient and hospitalised children ≤16 years in informal settlements in Nairobi County, Kenya.</p><p><strong>Methods: </strong>This study recruited 16,679 children aged ≤16 years who presented with salmonellosis symptoms for a period of 6 years (2013-2018). The patients were age-matched with controls (asymptomatic individuals). The study was conducted at 3 outpatient sites and 1 inpatient site; the outpatient sites were all located within the Mukuru informal settlement. The inpatient site was Mbagathi district hospital, which serves patients residing in Kibera informal settlement. Blood and stool samples from children with fever ≥38°C and/or diarrhea and stool samples alone from controls were collected for processing for the presence of iNTS using basic microbiology procedures including culture, serology, and Kirby Bauer disc diffusion for sensitivity testing. Dry blood spots were also taken and processed for sickle cell protein markers using high-performance liquid chromatography (HPLC). HIV and malaria tests were also conducted using rapid tests, respectively.</p><p><strong>Results: </strong>From the total of 22,246 blood and stool samples tested, 741 (3.3%) tested positive for <i>Salmonella</i> species. A total of 338 (45.6%) iNTS were isolated across all 4 sites; these consisted of 158 (21.3%) <i>Salmonella</i> Enteritidis and 180 (24.3%) <i>Salmonella</i> Typhimurium. The most common resistance phenotype was against ampicillin, chloramphenicol, and sulfamethoxazole trimethoprim. A total of 118 (34.9%) isolates were multidrug-resistant (MDR). Out of 2,684 dry blood samples subjected to HPLC for investigation of sickle cell disease traits, 1820 (67.8%) had normal haemoglobin (Hb AA/Hb AF); 162/2684 (6%) tested positive for sickle cell traits (Hb AS/Hb AFS). Some patients positive for iNTS were also found to have other co-morbidities; 4 (0.1%) tested positive for sickle cell disease (Hb FS), malaria, and HIV 8 (2.4%) and 5 (1.5%), respectively.</p><p><strong>Conclusion: </strong>The high prevalence of MDR iNTS isolates and emerging resistance to third-generation cephalosporins is of great concern, as they are the recommended drugs for the management of iNTS in our settings. Sickle cell disease, malaria, and HIV were all not major factors associated with iNTS disease among children in Mukuru and Kibera informal settlements.</p>","PeriodicalId":520284,"journal":{"name":"East Africa science","volume":"6 1","pages":"48-54"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11561362/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"East Africa science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24248/easci.v6i1.92","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Invasive non-typhoidal Salmonella (iNTS) disease continues to be a major public health problem, especially in sub-Saharan Africa (SSA), where incidence rates are 227 cases [range 152-341] per 100,000 populations. Populations at risk of iNTS include adults with human immunodeficiency virus (HIV) infection, malnourished children, and those with recent malaria or sickle-cell anaemia (SCA). In Kenya, iNTS disease is particularly a major challenge in poor informal settlements, with infants and young children less than 5 years of age being the most affected. Our study aimed to investigate the association between sickle cell disease, malaria, and HIV in multi-drug-resistant invasive non-typhoidal Salmonella from outpatient and hospitalised children ≤16 years in informal settlements in Nairobi County, Kenya.
Methods: This study recruited 16,679 children aged ≤16 years who presented with salmonellosis symptoms for a period of 6 years (2013-2018). The patients were age-matched with controls (asymptomatic individuals). The study was conducted at 3 outpatient sites and 1 inpatient site; the outpatient sites were all located within the Mukuru informal settlement. The inpatient site was Mbagathi district hospital, which serves patients residing in Kibera informal settlement. Blood and stool samples from children with fever ≥38°C and/or diarrhea and stool samples alone from controls were collected for processing for the presence of iNTS using basic microbiology procedures including culture, serology, and Kirby Bauer disc diffusion for sensitivity testing. Dry blood spots were also taken and processed for sickle cell protein markers using high-performance liquid chromatography (HPLC). HIV and malaria tests were also conducted using rapid tests, respectively.
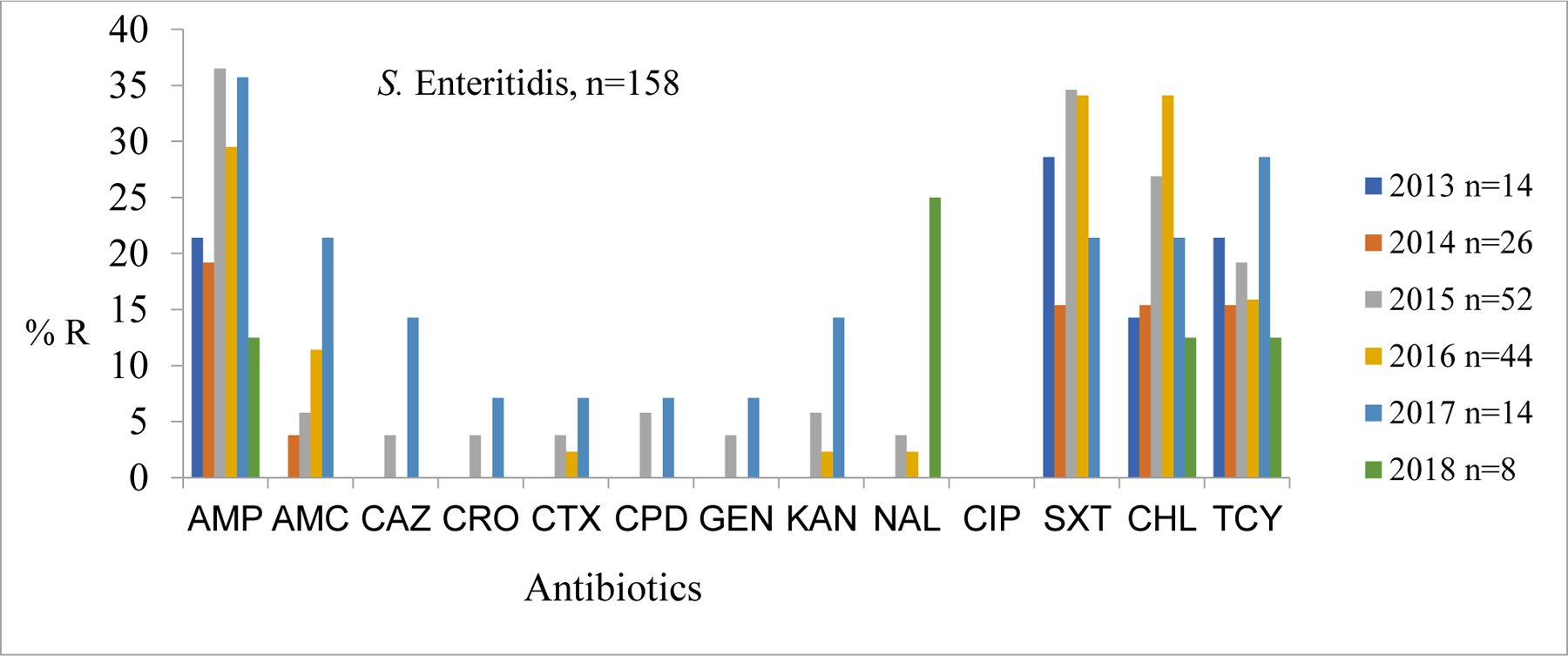
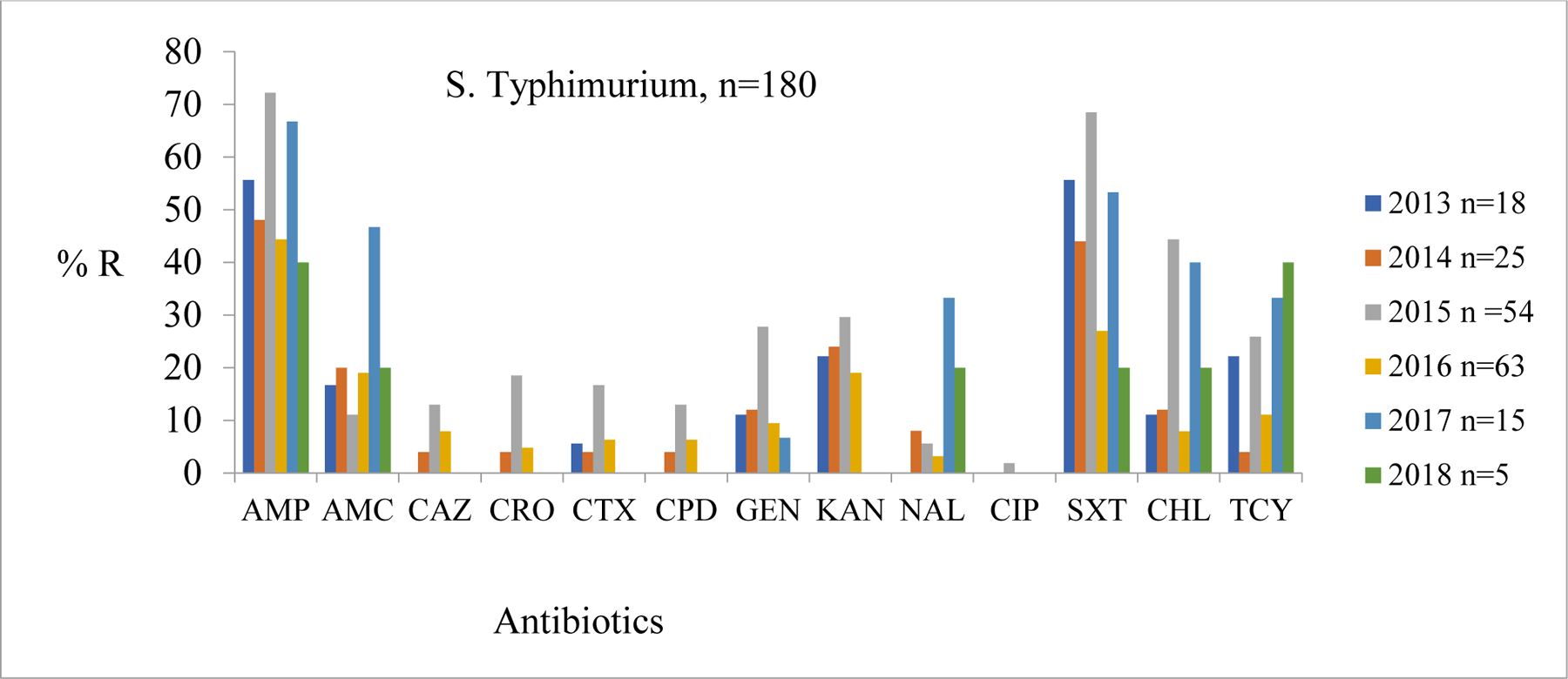
Results: From the total of 22,246 blood and stool samples tested, 741 (3.3%) tested positive for Salmonella species. A total of 338 (45.6%) iNTS were isolated across all 4 sites; these consisted of 158 (21.3%) Salmonella Enteritidis and 180 (24.3%) Salmonella Typhimurium. The most common resistance phenotype was against ampicillin, chloramphenicol, and sulfamethoxazole trimethoprim. A total of 118 (34.9%) isolates were multidrug-resistant (MDR). Out of 2,684 dry blood samples subjected to HPLC for investigation of sickle cell disease traits, 1820 (67.8%) had normal haemoglobin (Hb AA/Hb AF); 162/2684 (6%) tested positive for sickle cell traits (Hb AS/Hb AFS). Some patients positive for iNTS were also found to have other co-morbidities; 4 (0.1%) tested positive for sickle cell disease (Hb FS), malaria, and HIV 8 (2.4%) and 5 (1.5%), respectively.
Conclusion: The high prevalence of MDR iNTS isolates and emerging resistance to third-generation cephalosporins is of great concern, as they are the recommended drugs for the management of iNTS in our settings. Sickle cell disease, malaria, and HIV were all not major factors associated with iNTS disease among children in Mukuru and Kibera informal settlements.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
