Siju V Abraham, Anita Joy, Ankit Kumar Sahu, Prithvishree Ravindra, Shirshendu Dhar, Ravi Teja, S Vimal Krishnan, Renyu Liu, Anthony George Rudd, Gary A Ford
{"title":"Barriers to Effective Prehospital and Hyperacute Stroke Care in India: A Physician Perspective.","authors":"Siju V Abraham, Anita Joy, Ankit Kumar Sahu, Prithvishree Ravindra, Shirshendu Dhar, Ravi Teja, S Vimal Krishnan, Renyu Liu, Anthony George Rudd, Gary A Ford","doi":"10.4103/jets.jets_156_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The incidence of stroke is increasing in India. Prehospital stroke care is crucial for reducing stroke morbidity and mortality, but its implementation in India faces several challenges. Limited original research exists on prehospital stroke care in India, making it essential to identify the problems in implementing effective prehospital stroke care.</p><p><strong>Methods: </strong>A web-based survey was conducted among registered medical practitioners in India who treat acute stroke. The survey questionnaire was developed in English and included 26 questions divided into five parts: questions about the physician's practice setup/hospital in India, perception of community awareness, existing prehospital care/systems, in-hospital stroke care availability, and specific issues faced.</p><p><strong>Results: </strong>Eighty-three doctors in India participated in the survey (43% response rate). Most of the respondents worked in private hospitals (68%) and urban areas (76%). While 89% of hospitals had ambulance services, over 33% reported that patients had to pay for ambulance transport. Among respondents, 12% reported a community stroke care network, with infrequent prehospital procedures such as random blood glucose measurement (22%), stroke identification (15.7%), \"last seen normal\" documentation (14.5%), and low prehospital notification to hospitals (5%). Delays in referral from peripheral centers were reported by 73% of respondents. Most hospitals had standard operating procedures (SOPs) (84%), computed tomography (CT) (94%), magnetic resonance imaging (MRI) (85%), and offered intravenous thrombolysis (IVT) (77%). However, 24 h availability of CT was reported only by 6%, MRI by 19% and IVT by 12%. Nearly half (45%) reported treatment with thrombolysis was not covered by insurance. Mechanical thrombectomy was available in 34% of hospitals and 63% of hospitals conducted in-hospital audits for stroke patients.</p><p><strong>Conclusions: </strong>The capabilities of stroke-catering hospitals in urban settings are encouraging, with many having SOPs, imaging capabilities, and thrombolysis and mechanical thrombectomy services. However, there is much room for improvement, in making the essential stroke care services financially accessible to all and available around the clock.</p>","PeriodicalId":15692,"journal":{"name":"Journal of Emergencies, Trauma, and Shock","volume":"17 3","pages":"129-135"},"PeriodicalIF":0.7000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11563232/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Emergencies, Trauma, and Shock","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_156_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The incidence of stroke is increasing in India. Prehospital stroke care is crucial for reducing stroke morbidity and mortality, but its implementation in India faces several challenges. Limited original research exists on prehospital stroke care in India, making it essential to identify the problems in implementing effective prehospital stroke care.
Methods: A web-based survey was conducted among registered medical practitioners in India who treat acute stroke. The survey questionnaire was developed in English and included 26 questions divided into five parts: questions about the physician's practice setup/hospital in India, perception of community awareness, existing prehospital care/systems, in-hospital stroke care availability, and specific issues faced.
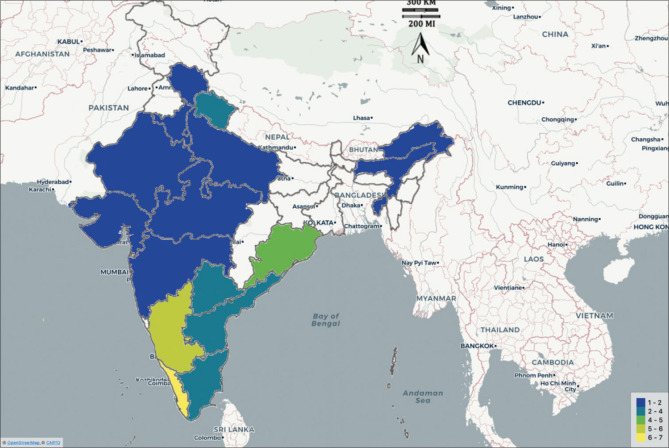
Results: Eighty-three doctors in India participated in the survey (43% response rate). Most of the respondents worked in private hospitals (68%) and urban areas (76%). While 89% of hospitals had ambulance services, over 33% reported that patients had to pay for ambulance transport. Among respondents, 12% reported a community stroke care network, with infrequent prehospital procedures such as random blood glucose measurement (22%), stroke identification (15.7%), "last seen normal" documentation (14.5%), and low prehospital notification to hospitals (5%). Delays in referral from peripheral centers were reported by 73% of respondents. Most hospitals had standard operating procedures (SOPs) (84%), computed tomography (CT) (94%), magnetic resonance imaging (MRI) (85%), and offered intravenous thrombolysis (IVT) (77%). However, 24 h availability of CT was reported only by 6%, MRI by 19% and IVT by 12%. Nearly half (45%) reported treatment with thrombolysis was not covered by insurance. Mechanical thrombectomy was available in 34% of hospitals and 63% of hospitals conducted in-hospital audits for stroke patients.
Conclusions: The capabilities of stroke-catering hospitals in urban settings are encouraging, with many having SOPs, imaging capabilities, and thrombolysis and mechanical thrombectomy services. However, there is much room for improvement, in making the essential stroke care services financially accessible to all and available around the clock.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
