Tara Ramaswamy , Michael P DeWane , Hassan S Dashti , Meghan Lau , Paul E Wischmeyer , Alexander Nagrebetsky , Jamie Sparling
{"title":"Nine Myths about Enteral Feeding in Critically Ill Adults: An Expert Perspective","authors":"Tara Ramaswamy , Michael P DeWane , Hassan S Dashti , Meghan Lau , Paul E Wischmeyer , Alexander Nagrebetsky , Jamie Sparling","doi":"10.1016/j.advnut.2024.100345","DOIUrl":null,"url":null,"abstract":"<div><div>Malnutrition is a well-studied and significant prognostic risk factor for morbidity and mortality in critically ill perioperative patients. Common nutrition myths in the critically ill may prevent early, consistent, and adequate delivery of enteral nutrition. We outlined 9 common intensive care unit (ICU) nutrition misconceptions and our recommendations to optimize enteral nutrition in critically ill patients based on the review of available literature. Our approach is to treat every patient admitted to the ICU as at risk for malnutrition and to initiate enteral nutrition upon admission in the absence of contraindications. Early enteral nutrition via the gastric route is more beneficial than delaying feeding while awaiting small bowel access and daytime-intermittent nutrition support can safely be initiated over continuous feeding. Gastric residual volumes to assess feeding tolerance should no longer be routinely measured. For perioperative nutrition, we recommend continuing enteral nutrition for most patients with secure airways undergoing anesthesia and resuming nutrition within 24 h of abdominal surgery; even patients with open abdomens can be safely fed in the absence of bowel injury. Critically ill patients who are proned, paralyzed, and on vasopressors can usually continue enteral nutrition. Finally, continuing enteral nutrition before extubation may optimize nutrition without compromising extubation success. In this review, we highlight several common misconceptions regarding ICU nutrition that may prevent achieving nutrition goals and subsequently lead to increased malnutrition, morbidity, and mortality. This knowledge may contribute to increased implementation of early and consistent enteral nutrition strategies to improve outcomes in critically ill adult patients.</div></div>","PeriodicalId":7349,"journal":{"name":"Advances in Nutrition","volume":"16 1","pages":"Article 100345"},"PeriodicalIF":9.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784768/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Nutrition","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2161831324001790","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
引用次数: 0
Abstract
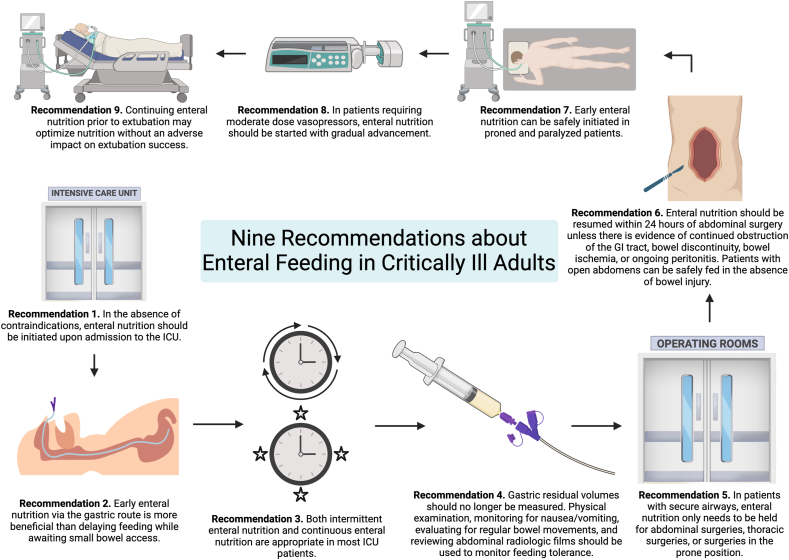
Malnutrition is a well-studied and significant prognostic risk factor for morbidity and mortality in critically ill perioperative patients. Common nutrition myths in the critically ill may prevent early, consistent, and adequate delivery of enteral nutrition. We outlined 9 common intensive care unit (ICU) nutrition misconceptions and our recommendations to optimize enteral nutrition in critically ill patients based on the review of available literature. Our approach is to treat every patient admitted to the ICU as at risk for malnutrition and to initiate enteral nutrition upon admission in the absence of contraindications. Early enteral nutrition via the gastric route is more beneficial than delaying feeding while awaiting small bowel access and daytime-intermittent nutrition support can safely be initiated over continuous feeding. Gastric residual volumes to assess feeding tolerance should no longer be routinely measured. For perioperative nutrition, we recommend continuing enteral nutrition for most patients with secure airways undergoing anesthesia and resuming nutrition within 24 h of abdominal surgery; even patients with open abdomens can be safely fed in the absence of bowel injury. Critically ill patients who are proned, paralyzed, and on vasopressors can usually continue enteral nutrition. Finally, continuing enteral nutrition before extubation may optimize nutrition without compromising extubation success. In this review, we highlight several common misconceptions regarding ICU nutrition that may prevent achieving nutrition goals and subsequently lead to increased malnutrition, morbidity, and mortality. This knowledge may contribute to increased implementation of early and consistent enteral nutrition strategies to improve outcomes in critically ill adult patients.
期刊介绍:
Advances in Nutrition (AN/Adv Nutr) publishes focused reviews on pivotal findings and recent research across all domains relevant to nutritional scientists and biomedical researchers. This encompasses nutrition-related research spanning biochemical, molecular, and genetic studies using experimental animal models, domestic animals, and human subjects. The journal also emphasizes clinical nutrition, epidemiology and public health, and nutrition education. Review articles concentrate on recent progress rather than broad historical developments.
In addition to review articles, AN includes Perspectives, Letters to the Editor, and supplements. Supplement proposals require pre-approval by the editor before submission. The journal features reports and position papers from the American Society for Nutrition, summaries of major government and foundation reports, and Nutrient Information briefs providing crucial details about dietary requirements, food sources, deficiencies, and other essential nutrient information. All submissions with scientific content undergo peer review by the Editors or their designees prior to acceptance for publication.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
