Health Economic Evaluation of Antimicrobial Stewardship, Procalcitonin Testing, and Rapid Blood Culture Identification in Sepsis Care: A 90-Day Model-Based, Cost-Utility Analysis.
Wendy I Sligl, Charles Yan, Jeff Round, Xiaoming Wang, Justin Z Chen, Cheyanne Boehm, Karen Fong, Katelynn Crick, Míriam Garrido Clua, Cassidy Codan, Tanis C Dingle, Connie Prosser, Guanmin Chen, Alena Tse-Chang, Daniel Garros, David Zygun, Dawn Opgenorth, John M Conly, Christopher J Doig, Vincent I Lau, Sean M Bagshaw
{"title":"Health Economic Evaluation of Antimicrobial Stewardship, Procalcitonin Testing, and Rapid Blood Culture Identification in Sepsis Care: A 90-Day Model-Based, Cost-Utility Analysis.","authors":"Wendy I Sligl, Charles Yan, Jeff Round, Xiaoming Wang, Justin Z Chen, Cheyanne Boehm, Karen Fong, Katelynn Crick, Míriam Garrido Clua, Cassidy Codan, Tanis C Dingle, Connie Prosser, Guanmin Chen, Alena Tse-Chang, Daniel Garros, David Zygun, Dawn Opgenorth, John M Conly, Christopher J Doig, Vincent I Lau, Sean M Bagshaw","doi":"10.1007/s41669-024-00538-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We evaluated the cost-effectiveness of a bundled intervention including an antimicrobial stewardship program (ASP), procalcitonin (PCT) testing, and rapid blood culture identification (BCID), compared with pre-implementation standard care in critically ill adult patients with sepsis.</p><p><strong>Methods: </strong>We conducted a decision tree model-based cost-effectiveness analysis alongside a previously published pre- and post-implementation quality improvement study. We adopted a public Canadian healthcare payer's perspective. Two intensive care units in Alberta with 727 adult critically ill patients were included. Our bundled intervention was compared with pre-implementation standard care. We collected healthcare resource use and estimated unit costs in 2022 Canadian dollars (CAD) over a time horizon from study entry to hospital discharge or death. We calculated the incremental net monetary benefit (iNMB) of the intervention group compared with the pre-intervention group. The primary outcome was cost per sepsis case. Secondary outcomes included readmission rates, Clostridioides difficile infections, mortality, and lengths of stay. Uncertainty was investigated using cost-effectiveness acceptability curves, cost-effectiveness plane scatterplots, and sensitivity analyses.</p><p><strong>Results: </strong>Mean (standard deviation [SD]) cost per index hospital admission was CAD $83,251 ($107,926) for patients in the intervention group and CAD $87,044 ($104,406) for the pre-intervention group, though the difference ($3,793 [$7,897]) was not statistically significant. Costs were higher in the pre-intervention group for antibiotics, readmissions, and C. difficile infections. The intervention group had a lower mean expected cost; $110,580 ($108,917) compared with pre-intervention ($125,745 [$113,210]), with a difference of $15,165 ($8278). There were no statistically significant differences in quality adjusted life years (QALYs) between groups. The iNMB of the intervention group compared with pre-intervention was greater than $15,000 for willingness-to-pay (WTP) per QALY values of between $0 and $100,000. In our sensitivity analysis, the intervention was most likely to be cost-effective in roughly 56% of simulations at all WTP thresholds.</p><p><strong>Conclusions: </strong>Our bundled intervention of ASP, PCT, and BCID among adult critically ill patients with sepsis was potentially cost-effective, but with substantial decision uncertainty.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"15-25"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11718022/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-024-00538-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: We evaluated the cost-effectiveness of a bundled intervention including an antimicrobial stewardship program (ASP), procalcitonin (PCT) testing, and rapid blood culture identification (BCID), compared with pre-implementation standard care in critically ill adult patients with sepsis.
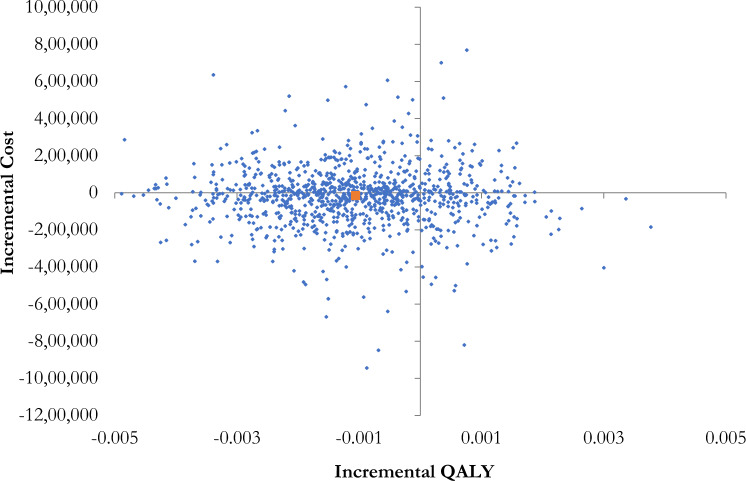
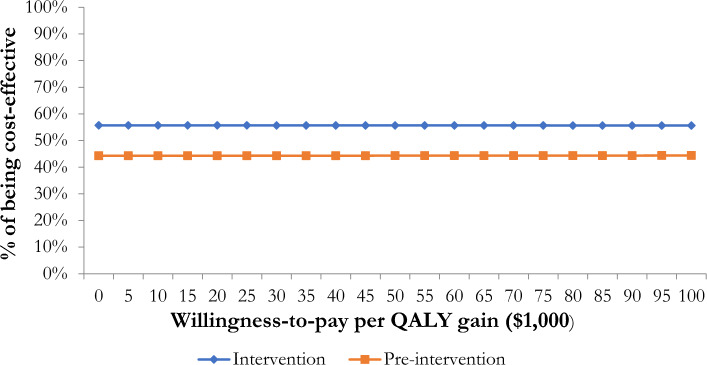
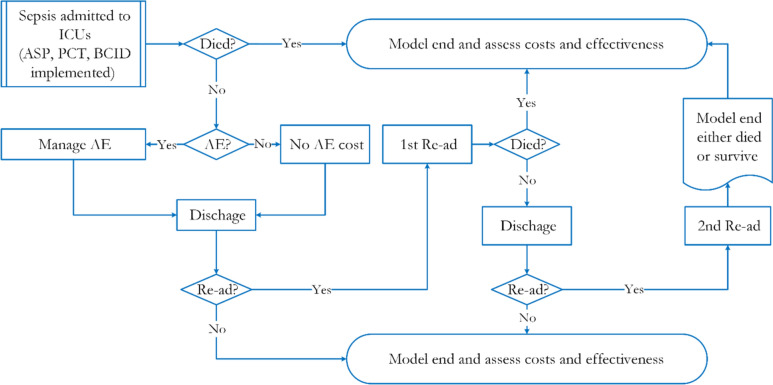
Methods: We conducted a decision tree model-based cost-effectiveness analysis alongside a previously published pre- and post-implementation quality improvement study. We adopted a public Canadian healthcare payer's perspective. Two intensive care units in Alberta with 727 adult critically ill patients were included. Our bundled intervention was compared with pre-implementation standard care. We collected healthcare resource use and estimated unit costs in 2022 Canadian dollars (CAD) over a time horizon from study entry to hospital discharge or death. We calculated the incremental net monetary benefit (iNMB) of the intervention group compared with the pre-intervention group. The primary outcome was cost per sepsis case. Secondary outcomes included readmission rates, Clostridioides difficile infections, mortality, and lengths of stay. Uncertainty was investigated using cost-effectiveness acceptability curves, cost-effectiveness plane scatterplots, and sensitivity analyses.
Results: Mean (standard deviation [SD]) cost per index hospital admission was CAD $83,251 ($107,926) for patients in the intervention group and CAD $87,044 ($104,406) for the pre-intervention group, though the difference ($3,793 [$7,897]) was not statistically significant. Costs were higher in the pre-intervention group for antibiotics, readmissions, and C. difficile infections. The intervention group had a lower mean expected cost; $110,580 ($108,917) compared with pre-intervention ($125,745 [$113,210]), with a difference of $15,165 ($8278). There were no statistically significant differences in quality adjusted life years (QALYs) between groups. The iNMB of the intervention group compared with pre-intervention was greater than $15,000 for willingness-to-pay (WTP) per QALY values of between $0 and $100,000. In our sensitivity analysis, the intervention was most likely to be cost-effective in roughly 56% of simulations at all WTP thresholds.
Conclusions: Our bundled intervention of ASP, PCT, and BCID among adult critically ill patients with sepsis was potentially cost-effective, but with substantial decision uncertainty.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
