{"title":"Real-world clinical data-driven modelling on the initiation time of antiviral prophylaxis among pregnant women with chronic hepatitis B infection","authors":"Mingwang Shen, Shihao He, Naijuan Yao, Rui Li, Jing Wang, Wenting Zhong, Jinyan Wang, Huihui Wang, Li Xie, Guihua Zhuang, Lei Zhang, Tianyan Chen","doi":"10.1016/j.jhep.2024.11.017","DOIUrl":null,"url":null,"abstract":"<h3>Background & Aims</h3>The risk of mother-to-child transmission (MTCT) for pregnant women with chronic hepatitis B (CHB) infection still exists, especially for those with high HBV DNA level. The guidelines for initiating prophylaxis for pregnant women with CHB vary across countries. We aimed to explore the latest prophylaxis initiation time for these women.<h3>Methods</h3>We collected the real-world clinical data of 328 pregnant women with CHB infection aged 20-49 treated by telbivudine (LdT) or tenofovir disoproxil fumarate (TDF) from July 2010 to December 2020 in China. A mathematical model was developed to describe the viral kinetics of HBV after prophylaxis. We calculated the time required to reduce viral load below the threshold value of 5.3 log<sub>10</sub> IU/mL. We derived the prophylaxis initiation time by subtracting the required time to threshold from the childbirth gestational week.<h3>Results</h3>The median time for 328 women to reduce HBV DNA levels below the threshold of 5.3 log<sub>10</sub> IU/mL was 4.2 (range: 0.2-12.8) weeks, corresponding to prophylaxis initiation time of no later than 35.1 (25.2-41.4) weeks. Specifically, for women with viral loads > 8.0 log<sub>10</sub> IU/mL, prophylaxis should be initiated before 33.9 (25.2-39.5) weeks, and particularly before the lower bound of 25.2 weeks, to maximize clinical safety. For women with viral load >7.0 to <span><span style=\"display: none;\"></span><span data-mathml='<math xmlns=\"http://www.w3.org/1998/Math/MathML\"><mrow is=\"true\"><mo linebreak=\"goodbreak\" linebreakstyle=\"after\" is=\"true\">&#x2264;</mo></mrow></math>' role=\"presentation\" style=\"position: relative;\" tabindex=\"0\"><span aria-hidden=\"true\">[Math Processing Error]</span><span role=\"presentation\"><math xmlns=\"http://www.w3.org/1998/Math/MathML\"><mrow is=\"true\"><mo is=\"true\" linebreak=\"goodbreak\" linebreakstyle=\"after\">≤</mo></mrow></math></span></span><script type=\"math/mml\"><math><mrow is=\"true\"><mo linebreak=\"goodbreak\" linebreakstyle=\"after\" is=\"true\">≤</mo></mrow></math></script></span> 8.0 log<sub>10</sub> IU/mL, prophylaxis should be initiated before 35.5 (28.6-39.8) weeks, and for women with viral load >5.3 to <span><span style=\"display: none;\"></span><span data-mathml='<math xmlns=\"http://www.w3.org/1998/Math/MathML\"><mrow is=\"true\"><mo linebreak=\"goodbreak\" linebreakstyle=\"after\" is=\"true\">&#x2264;</mo></mrow></math>' role=\"presentation\" style=\"position: relative;\" tabindex=\"0\"><span aria-hidden=\"true\">[Math Processing Error]</span><span role=\"presentation\"><math xmlns=\"http://www.w3.org/1998/Math/MathML\"><mrow is=\"true\"><mo is=\"true\" linebreak=\"goodbreak\" linebreakstyle=\"after\">≤</mo></mrow></math></span></span><script type=\"math/mml\"><math><mrow is=\"true\"><mo linebreak=\"goodbreak\" linebreakstyle=\"after\" is=\"true\">≤</mo></mrow></math></script></span> 7.0 log<sub>10</sub> IU/mL, prophylaxis should be initiated before 36.2 (28.3-41.4) weeks.<h3>Conclusion</h3>Pregnant women with HBV DNA levels >5.3 to <span><span style=\"display: none;\"></span><span data-mathml='<math xmlns=\"http://www.w3.org/1998/Math/MathML\"><mrow is=\"true\"><mo linebreak=\"goodbreak\" linebreakstyle=\"after\" is=\"true\">&#x2264;</mo></mrow></math>' role=\"presentation\" style=\"position: relative;\" tabindex=\"0\"><span aria-hidden=\"true\">[Math Processing Error]</span><span role=\"presentation\"><math xmlns=\"http://www.w3.org/1998/Math/MathML\"><mrow is=\"true\"><mo is=\"true\" linebreak=\"goodbreak\" linebreakstyle=\"after\">≤</mo></mrow></math></span></span><script type=\"math/mml\"><math><mrow is=\"true\"><mo linebreak=\"goodbreak\" linebreakstyle=\"after\" is=\"true\">≤</mo></mrow></math></script></span> 8.0 log<sub>10</sub> IU/mL can initiate prophylaxis before 28 gestational weeks. However, women with HBV DNA >8.0 log<sub>10</sub> IU/mL could consider initiating prophylaxis before 25 weeks.<h3>Impact and implications</h3>This study investigates how long it takes to decrease maternal viral load below a threshold·(5.3 log<sub>10</sub> IU/mL) after receiving antiviral prophylaxis in pregnant women with different HBV DNA levels based on real-world clinical data and mathematical modelling, which provides quantitative evidence on the initiation time of antiviral prophylaxis. The results show that pregnant women with CHB infection at high HBV DNA levels (>8 log<sub>10</sub> IU/mL) should initiate antiviral prophylaxis earlier to decrease the risk of mother-to-child transmission of HBV. Physicians can determine when to begin antiviral prophylaxis for those women according to their maternal HBV DNA levels. Our findings justify the initiation time of antiviral prophylaxis recommended by the Chinese guidelines and will offer new insights for other international guidelines.","PeriodicalId":15888,"journal":{"name":"Journal of Hepatology","volume":"16 1","pages":""},"PeriodicalIF":26.8000,"publicationDate":"2024-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jhep.2024.11.017","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background & Aims
The risk of mother-to-child transmission (MTCT) for pregnant women with chronic hepatitis B (CHB) infection still exists, especially for those with high HBV DNA level. The guidelines for initiating prophylaxis for pregnant women with CHB vary across countries. We aimed to explore the latest prophylaxis initiation time for these women.
Methods
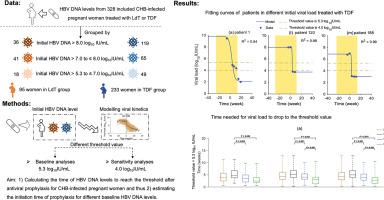
We collected the real-world clinical data of 328 pregnant women with CHB infection aged 20-49 treated by telbivudine (LdT) or tenofovir disoproxil fumarate (TDF) from July 2010 to December 2020 in China. A mathematical model was developed to describe the viral kinetics of HBV after prophylaxis. We calculated the time required to reduce viral load below the threshold value of 5.3 log10 IU/mL. We derived the prophylaxis initiation time by subtracting the required time to threshold from the childbirth gestational week.
Results
The median time for 328 women to reduce HBV DNA levels below the threshold of 5.3 log10 IU/mL was 4.2 (range: 0.2-12.8) weeks, corresponding to prophylaxis initiation time of no later than 35.1 (25.2-41.4) weeks. Specifically, for women with viral loads > 8.0 log10 IU/mL, prophylaxis should be initiated before 33.9 (25.2-39.5) weeks, and particularly before the lower bound of 25.2 weeks, to maximize clinical safety. For women with viral load >7.0 to [Math Processing Error] 8.0 log10 IU/mL, prophylaxis should be initiated before 35.5 (28.6-39.8) weeks, and for women with viral load >5.3 to [Math Processing Error] 7.0 log10 IU/mL, prophylaxis should be initiated before 36.2 (28.3-41.4) weeks.
Conclusion
Pregnant women with HBV DNA levels >5.3 to [Math Processing Error] 8.0 log10 IU/mL can initiate prophylaxis before 28 gestational weeks. However, women with HBV DNA >8.0 log10 IU/mL could consider initiating prophylaxis before 25 weeks.
Impact and implications
This study investigates how long it takes to decrease maternal viral load below a threshold·(5.3 log10 IU/mL) after receiving antiviral prophylaxis in pregnant women with different HBV DNA levels based on real-world clinical data and mathematical modelling, which provides quantitative evidence on the initiation time of antiviral prophylaxis. The results show that pregnant women with CHB infection at high HBV DNA levels (>8 log10 IU/mL) should initiate antiviral prophylaxis earlier to decrease the risk of mother-to-child transmission of HBV. Physicians can determine when to begin antiviral prophylaxis for those women according to their maternal HBV DNA levels. Our findings justify the initiation time of antiviral prophylaxis recommended by the Chinese guidelines and will offer new insights for other international guidelines.
期刊介绍:
The Journal of Hepatology is the official publication of the European Association for the Study of the Liver (EASL). It is dedicated to presenting clinical and basic research in the field of hepatology through original papers, reviews, case reports, and letters to the Editor. The Journal is published in English and may consider supplements that pass an editorial review.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
