The Effect of Everolimus Versus Calcineurin Inhibitors on Quality of Life 10–12 Years After Heart Transplantation: The Results of a Randomized Controlled Trial (SCHEDULE Trial)
Ingelin Grov, Anne Relbo Authen, Satish Arora, Niklas Bergh, Katrine Rolid, Finn Gustafsson, Hans Eiskjær, Göran Rådegran, Einar Gude, Arne K. Andreassen, Thea Halden, Kaspar Broch, Lars Gullestad, the SCHEDULE investigators
{"title":"The Effect of Everolimus Versus Calcineurin Inhibitors on Quality of Life 10–12 Years After Heart Transplantation: The Results of a Randomized Controlled Trial (SCHEDULE Trial)","authors":"Ingelin Grov, Anne Relbo Authen, Satish Arora, Niklas Bergh, Katrine Rolid, Finn Gustafsson, Hans Eiskjær, Göran Rådegran, Einar Gude, Arne K. Andreassen, Thea Halden, Kaspar Broch, Lars Gullestad, the SCHEDULE investigators","doi":"10.1111/ctr.70028","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Calcineurin inhibitors (CNIs) are associated with long-term complications after heart transplantation (HTx). Everolimus (EVR)-based immunosuppression allows for CNI withdrawal. We used data from The Scandinavian heart transplant everolimus de novo study with early CNI avoidance (SCHEDULE) trial to assess whether health-related quality of life (HRQoL) differed between patients on long-term treatment with EVR versus a CNI-based regimen.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>In SCHEDULE, we randomized 115 patients (mean age 51 ± 13 years, 27% women) to cyclosporine (CNI group; <i>n</i> = 59), or early introduction of EVR and cyclosporine withdrawal within 11 weeks of HTx (EVR group; <i>n</i> = 56). The primary endpoint was the glomerular filtration rate. We used the Short Form-36 (SF-36v2), the EuroQoL visual analogue scale (EQ VAS), and the Beck Depression Inventory (BDI) to assess HRQoL. We re-evaluated the participants after 10–12 years.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Seventy-eight patients attended follow-up at a median of 11 years after HTx. The SF-36 physical component summary score increased from 32 ± 10 pre-HTx to 44 ± 12 11 years after HTx (<i>p</i> < 0.01) in the EVR group and from 33 ± 9 to 44 ± 11 (<i>p</i> < 0.01) with CNI. The mental component summary score increased from 46 ± 12 to 53 ± 13 (EVR); <i>p</i> = 0.04 and from 38 ± 13 to 49 ± 13 (CNI); <i>p</i> < 0.01. Similar improvements were observed regarding EQ-VAS and the BDI. There were no significant between-group differences for either measure of HRQoL.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>In heart transplant recipients, an EVR-based immunosuppressive strategy resulted in similar long-term improvements in HRQoL as treatment with a CNI-based regimen.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"38 11","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11582939/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70028","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Calcineurin inhibitors (CNIs) are associated with long-term complications after heart transplantation (HTx). Everolimus (EVR)-based immunosuppression allows for CNI withdrawal. We used data from The Scandinavian heart transplant everolimus de novo study with early CNI avoidance (SCHEDULE) trial to assess whether health-related quality of life (HRQoL) differed between patients on long-term treatment with EVR versus a CNI-based regimen.
Methods
In SCHEDULE, we randomized 115 patients (mean age 51 ± 13 years, 27% women) to cyclosporine (CNI group; n = 59), or early introduction of EVR and cyclosporine withdrawal within 11 weeks of HTx (EVR group; n = 56). The primary endpoint was the glomerular filtration rate. We used the Short Form-36 (SF-36v2), the EuroQoL visual analogue scale (EQ VAS), and the Beck Depression Inventory (BDI) to assess HRQoL. We re-evaluated the participants after 10–12 years.
Results
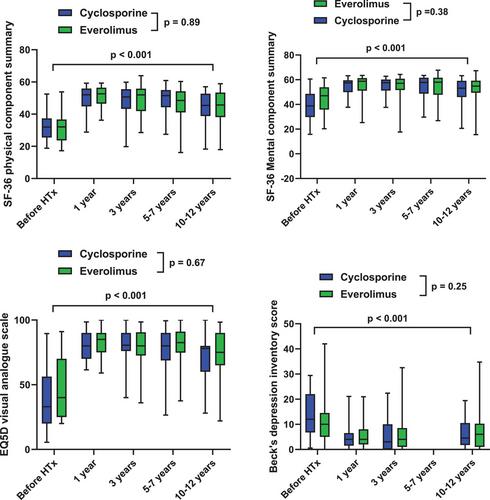
Seventy-eight patients attended follow-up at a median of 11 years after HTx. The SF-36 physical component summary score increased from 32 ± 10 pre-HTx to 44 ± 12 11 years after HTx (p < 0.01) in the EVR group and from 33 ± 9 to 44 ± 11 (p < 0.01) with CNI. The mental component summary score increased from 46 ± 12 to 53 ± 13 (EVR); p = 0.04 and from 38 ± 13 to 49 ± 13 (CNI); p < 0.01. Similar improvements were observed regarding EQ-VAS and the BDI. There were no significant between-group differences for either measure of HRQoL.
Conclusions
In heart transplant recipients, an EVR-based immunosuppressive strategy resulted in similar long-term improvements in HRQoL as treatment with a CNI-based regimen.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
