Clonal hematopoiesis of indeterminate potential is associated with increased risk of immune checkpoint inhibitor myocarditis in a prospective study of a cardio-oncology cohort.
Rachel Jaber Chehayeb, Jaiveer Singh, Carlos Matute-Martinez, Nathan W Chen, Ana Ferrigno Guajardo, Derrick Lin, Ritujith Jayakrishnan, Anthos Christofides, Etienne Leveille, Yunju Im, Giulia Biancon, Jennifer VanOudenhove, Eiman Ibrahim, Anastasias Ardasheva, Alokkumar Jha, John Hwa, Stephanie Halene, Jennifer M Kwan
{"title":"Clonal hematopoiesis of indeterminate potential is associated with increased risk of immune checkpoint inhibitor myocarditis in a prospective study of a cardio-oncology cohort.","authors":"Rachel Jaber Chehayeb, Jaiveer Singh, Carlos Matute-Martinez, Nathan W Chen, Ana Ferrigno Guajardo, Derrick Lin, Ritujith Jayakrishnan, Anthos Christofides, Etienne Leveille, Yunju Im, Giulia Biancon, Jennifer VanOudenhove, Eiman Ibrahim, Anastasias Ardasheva, Alokkumar Jha, John Hwa, Stephanie Halene, Jennifer M Kwan","doi":"10.1186/s40959-024-00289-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clonal hematopoiesis of indeterminate potential (CHIP) has been shown to increase all-cause mortality and risk of cardiomyopathy in patients with solid malignancies. CHIP has also been shown to increase T cell activation in heart failure patients. It is unclear whether CHIP can affect the risk of immune checkpoint inhibitor (ICI) myocarditis in patients with cancer treated with immunotherapy.</p><p><strong>Methods: </strong>We enrolled patients with solid tumors in a prospective study, determined CHIP status at time of enrollment through blood whole exome sequencing, and assessed incidence of ICI myocarditis from time of enrollment through December 1st, 2023. We performed a competing risk cox regression to evaluate the role of CHIP in ICI myocarditis, accounting for patient demographics, cardiac comorbidities, cardiotoxic cancer therapy, and dual ICI use in our covariates. We also generated cumulative incidence curves using subdistribution hazards to evaluate development of ICI myocarditis stratified by CHIP vs no CHIP. Chart review was performed to evaluate patient co-morbidities, lab values, imaging findings and outcomes.</p><p><strong>Results: </strong>Among the 88 patients receiving ICI therapy, average age was 67 ± 14 years, of which 50% harbored CHIP variants. Among all comorbidities, including diabetes, heart failure and obstructive coronary artery disease, only coronary artery calcifications were significantly increased in patients with CHIP. There were no statistically significant differences in cancer therapy or cardiovascular drugs between patients with and without CHIP. Among examined outcomes, patients with CHIP had a statistically higher rate of ICI myocarditis (overall: 57%, CHIP: 73% (32/44), no CHIP: 41% (18/44), p = 0.003) and death (CHIP: 60%, no CHIP 31%, p = 0.011). In a multivariate competing risk analysis, CHIP status doubled the risk of developing ICI myocarditis, similar to the risk of dual ICI use (CHIP status HR 2.74, 95% CI: 1.44-5.22, p = 0.002 vs dual ICI use HR 2.39, 95% CI: 1.11-5.14, p = 0.026).</p><p><strong>Conclusions: </strong>This study is the first to show that CHIP independently increases risk of ICI myocarditis, with implications for risk stratification of patients prior to ICI initiation and frequency of cardiac monitoring.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"84"},"PeriodicalIF":3.2000,"publicationDate":"2024-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11590368/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00289-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Clonal hematopoiesis of indeterminate potential (CHIP) has been shown to increase all-cause mortality and risk of cardiomyopathy in patients with solid malignancies. CHIP has also been shown to increase T cell activation in heart failure patients. It is unclear whether CHIP can affect the risk of immune checkpoint inhibitor (ICI) myocarditis in patients with cancer treated with immunotherapy.
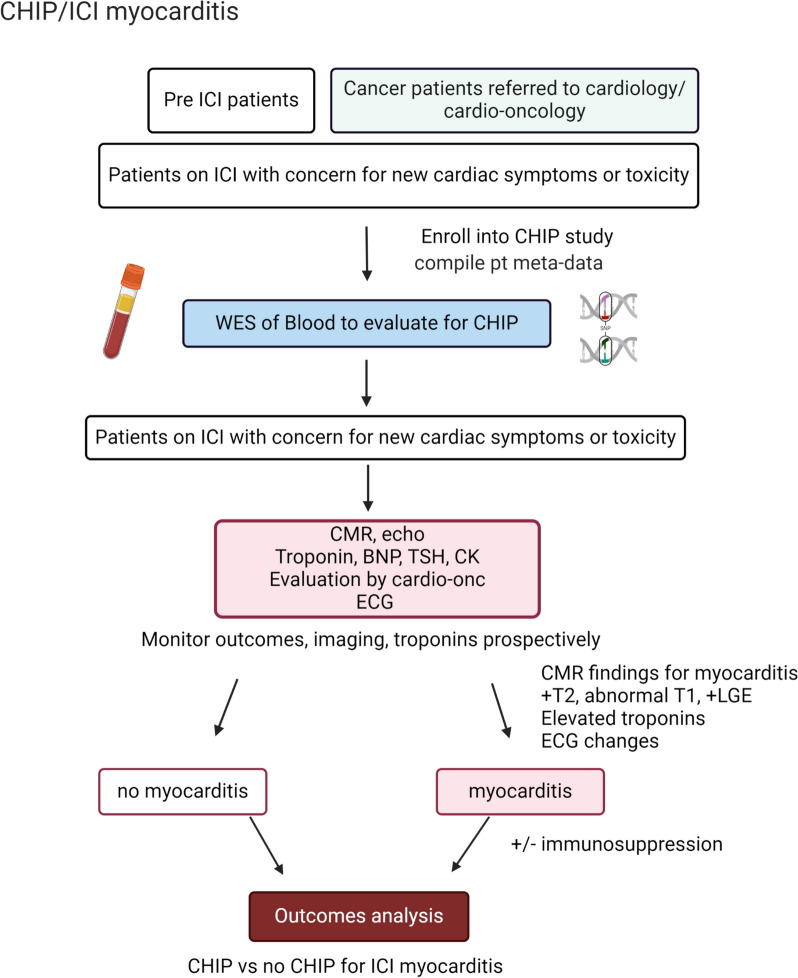
Methods: We enrolled patients with solid tumors in a prospective study, determined CHIP status at time of enrollment through blood whole exome sequencing, and assessed incidence of ICI myocarditis from time of enrollment through December 1st, 2023. We performed a competing risk cox regression to evaluate the role of CHIP in ICI myocarditis, accounting for patient demographics, cardiac comorbidities, cardiotoxic cancer therapy, and dual ICI use in our covariates. We also generated cumulative incidence curves using subdistribution hazards to evaluate development of ICI myocarditis stratified by CHIP vs no CHIP. Chart review was performed to evaluate patient co-morbidities, lab values, imaging findings and outcomes.
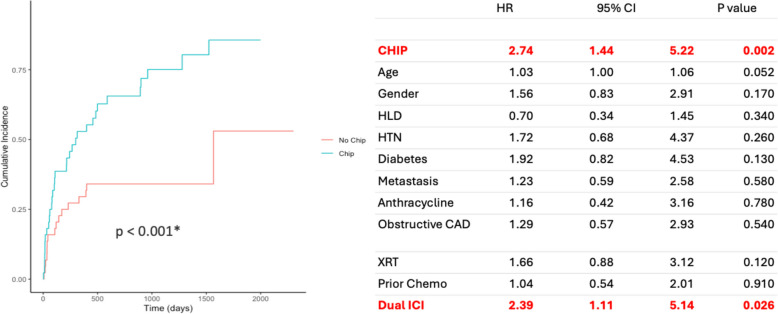
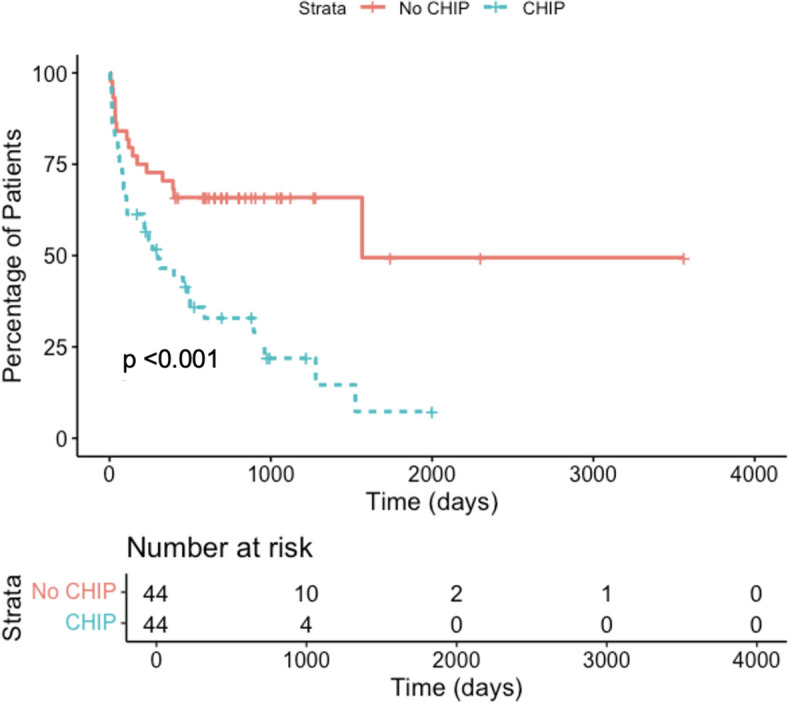
Results: Among the 88 patients receiving ICI therapy, average age was 67 ± 14 years, of which 50% harbored CHIP variants. Among all comorbidities, including diabetes, heart failure and obstructive coronary artery disease, only coronary artery calcifications were significantly increased in patients with CHIP. There were no statistically significant differences in cancer therapy or cardiovascular drugs between patients with and without CHIP. Among examined outcomes, patients with CHIP had a statistically higher rate of ICI myocarditis (overall: 57%, CHIP: 73% (32/44), no CHIP: 41% (18/44), p = 0.003) and death (CHIP: 60%, no CHIP 31%, p = 0.011). In a multivariate competing risk analysis, CHIP status doubled the risk of developing ICI myocarditis, similar to the risk of dual ICI use (CHIP status HR 2.74, 95% CI: 1.44-5.22, p = 0.002 vs dual ICI use HR 2.39, 95% CI: 1.11-5.14, p = 0.026).
Conclusions: This study is the first to show that CHIP independently increases risk of ICI myocarditis, with implications for risk stratification of patients prior to ICI initiation and frequency of cardiac monitoring.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
