{"title":"Evidence for Aldosterone Antagonism in Heart Failure.","authors":"Rishi Sethi, Pravesh Vishwakarma, Akshyaya Pradhan","doi":"10.15420/cfr.2024.10","DOIUrl":null,"url":null,"abstract":"<p><p>Activation of the renin-angiotensin-aldosterone system is the ultimate pathophysiological hallmark in heart failure. Though aldosterone primarily appears to regulate electrolyte homeostasis by acting on distal nephrons in the kidneys, its effects are far-reaching across the cardiovascular system as its receptors are also expressed in vascular smooth muscle cells, endothelial cells, macrophages and cardiomyocytes. Aldosterone excess leads to vascular stiffness, vasoconstriction, endothelial dysfunction, inflammation, oxidative stress, cardiac fibrosis and hypertrophy, atherogenesis and thrombosis. Hence, aldosterone antagonism is an attractive proposition for heart failure management. The first-generation non-selective mineralocorticoid receptor antagonist spironolactone produced a spectacular reduction of cardiovascular outcomes in the seminal RALES study, while the selective second-generation congener eplerenone boasts two positive studies: EPHESUS and EMPHASIS-HF. The TOPCAT trial indicated that a specific subgroup of patients with heart failure with preserved ejection fraction may benefit from targeted therapy of mineralocorticoid receptor antagonists. Newer-generation non-steroidal mineralocorticoid antagonists and aldosterone synthase inhibitors are being evaluated in randomised trials.</p>","PeriodicalId":33741,"journal":{"name":"Cardiac Failure Review","volume":"10 ","pages":"e15"},"PeriodicalIF":5.7000,"publicationDate":"2024-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11588114/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiac Failure Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/cfr.2024.10","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
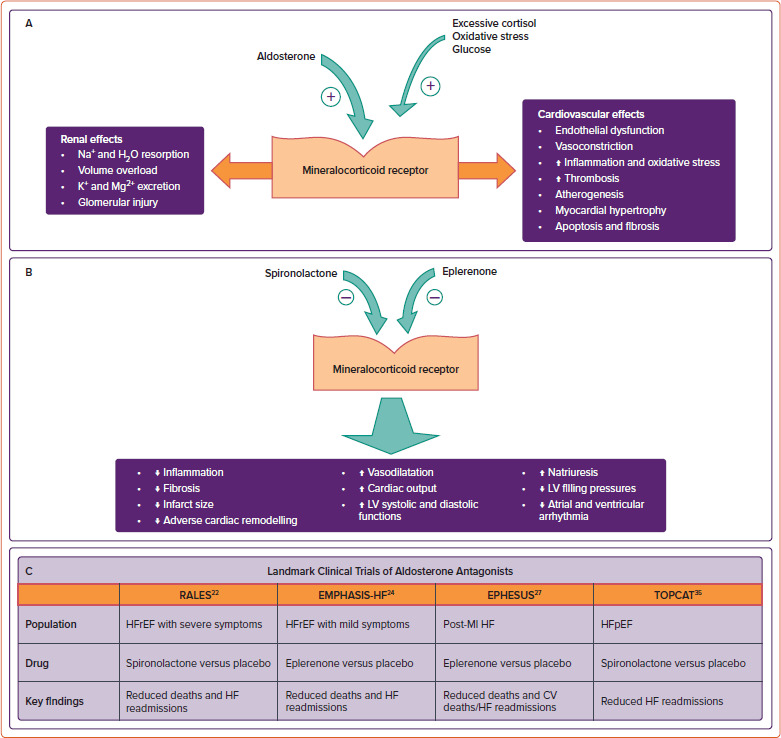
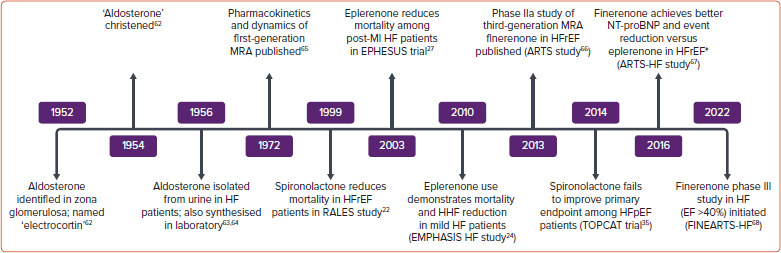
Activation of the renin-angiotensin-aldosterone system is the ultimate pathophysiological hallmark in heart failure. Though aldosterone primarily appears to regulate electrolyte homeostasis by acting on distal nephrons in the kidneys, its effects are far-reaching across the cardiovascular system as its receptors are also expressed in vascular smooth muscle cells, endothelial cells, macrophages and cardiomyocytes. Aldosterone excess leads to vascular stiffness, vasoconstriction, endothelial dysfunction, inflammation, oxidative stress, cardiac fibrosis and hypertrophy, atherogenesis and thrombosis. Hence, aldosterone antagonism is an attractive proposition for heart failure management. The first-generation non-selective mineralocorticoid receptor antagonist spironolactone produced a spectacular reduction of cardiovascular outcomes in the seminal RALES study, while the selective second-generation congener eplerenone boasts two positive studies: EPHESUS and EMPHASIS-HF. The TOPCAT trial indicated that a specific subgroup of patients with heart failure with preserved ejection fraction may benefit from targeted therapy of mineralocorticoid receptor antagonists. Newer-generation non-steroidal mineralocorticoid antagonists and aldosterone synthase inhibitors are being evaluated in randomised trials.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
