Miguel Miranda, Joana Polido, Miguel Fernandes, Filipe Lopes, Tiago Oliveira, Tomé Lopes, Luís Costa, Ângelo Nobre, Tito Palmela Leitão, Luís Mendes Pedro, José Palma Dos Reis
{"title":"Renal cell carcinoma with inferior vena cava thrombus: Survival and prognostic factors in surgically treated patients.","authors":"Miguel Miranda, Joana Polido, Miguel Fernandes, Filipe Lopes, Tiago Oliveira, Tomé Lopes, Luís Costa, Ângelo Nobre, Tito Palmela Leitão, Luís Mendes Pedro, José Palma Dos Reis","doi":"10.4103/ua.ua_113_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Renal cell carcinoma (RCC) often develops a tumor thrombus extending into the inferior vena cava (IVC). Radical nephrectomy with IVC thrombectomy is the standard treatment, although prognostic factors are yet to be properly established.</p><p><strong>Objectives: </strong>The objectives of this study were to review the clinicopathological features of surgically treated patients with RCC and IVC thrombus and to investigate potential prognostic factors.</p><p><strong>Materials and methods: </strong>This retrospective analysis covered patients with RCC and IVC thrombus who underwent surgical treatment at a tertiary center over 12 years.</p><p><strong>Results: </strong>Of the 32 patients included, 56% and 41% had nodal (N1) and metastatic (M1) diseases, respectively. Thrombus level was 1 in 25% and 4 in 21.9% of cases, according to the Mayo classification. The median follow-up was 17.0 months. The median overall survival (OS) was 20.0 months, with a median OS of 36.0 months in M0 patients and 10.0 months in M1 patients (log-rank <i>P</i> = 0.029). Stage IV disease (T4 and/or M1 status) (hazard ratio [HR]: 2.85, <i>P</i> = 0.021), fat invasion (HR: 2.52, <i>P</i> = 0.044), positive margins (HR: 2.54, <i>P</i> = 0.037), American Society of Anesthesiologists score (HR: 2.59, <i>P</i> = 0.033), tumor size >100 mm (HR: 2.538, <i>P</i> = 0.033), and higher neutrophil-to-lymphocyte ratio (<i>r</i> <sup>2</sup> = 0.304, <i>P</i> = 0.001) were significantly associated with worse OS in univariate analysis. Thrombus level did not impact prognosis.</p><p><strong>Conclusions: </strong>Certain clinicopathological factors, but not thrombus level, appear to influence prognosis. Prospective multicentric randomized studies are needed to better stratify patient risk, improve prognostic prediction, and evaluate systemic therapy responses.</p>","PeriodicalId":23633,"journal":{"name":"Urology Annals","volume":"16 4","pages":"277-283"},"PeriodicalIF":0.8000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587942/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology Annals","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ua.ua_113_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/16 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Renal cell carcinoma (RCC) often develops a tumor thrombus extending into the inferior vena cava (IVC). Radical nephrectomy with IVC thrombectomy is the standard treatment, although prognostic factors are yet to be properly established.
Objectives: The objectives of this study were to review the clinicopathological features of surgically treated patients with RCC and IVC thrombus and to investigate potential prognostic factors.
Materials and methods: This retrospective analysis covered patients with RCC and IVC thrombus who underwent surgical treatment at a tertiary center over 12 years.
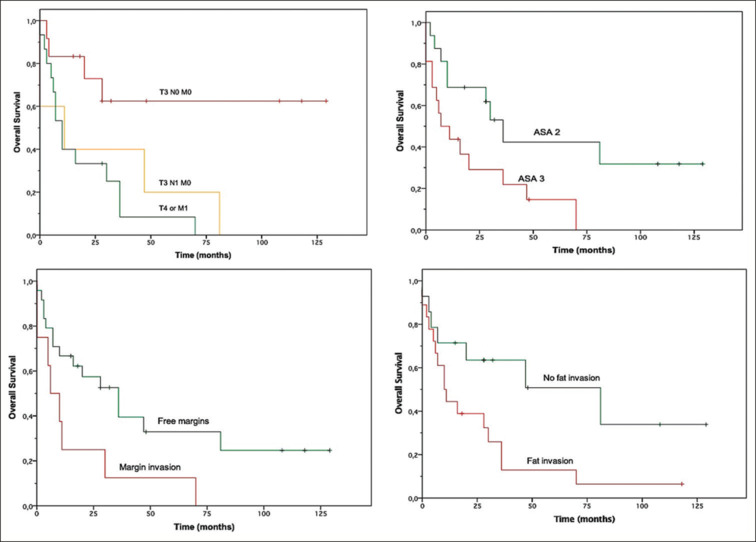
Results: Of the 32 patients included, 56% and 41% had nodal (N1) and metastatic (M1) diseases, respectively. Thrombus level was 1 in 25% and 4 in 21.9% of cases, according to the Mayo classification. The median follow-up was 17.0 months. The median overall survival (OS) was 20.0 months, with a median OS of 36.0 months in M0 patients and 10.0 months in M1 patients (log-rank P = 0.029). Stage IV disease (T4 and/or M1 status) (hazard ratio [HR]: 2.85, P = 0.021), fat invasion (HR: 2.52, P = 0.044), positive margins (HR: 2.54, P = 0.037), American Society of Anesthesiologists score (HR: 2.59, P = 0.033), tumor size >100 mm (HR: 2.538, P = 0.033), and higher neutrophil-to-lymphocyte ratio (r2 = 0.304, P = 0.001) were significantly associated with worse OS in univariate analysis. Thrombus level did not impact prognosis.
Conclusions: Certain clinicopathological factors, but not thrombus level, appear to influence prognosis. Prospective multicentric randomized studies are needed to better stratify patient risk, improve prognostic prediction, and evaluate systemic therapy responses.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
