Prospective phase II study of allogeneic hematopoietic stem cell transplantation with targeted busulfan, fludarabine, and etoposide conditioning in pediatric acute lymphoblastic leukemia
Kyung Taek Hong, Hyun Jin Park, Bo Kyung Kim, Jung Yoon Choi, Sang Hoon Song, SeungHwan Lee, Kyung-Sang Yu, In-Jin Jang, Hyoung Jin Kang
{"title":"Prospective phase II study of allogeneic hematopoietic stem cell transplantation with targeted busulfan, fludarabine, and etoposide conditioning in pediatric acute lymphoblastic leukemia","authors":"Kyung Taek Hong, Hyun Jin Park, Bo Kyung Kim, Jung Yoon Choi, Sang Hoon Song, SeungHwan Lee, Kyung-Sang Yu, In-Jin Jang, Hyoung Jin Kang","doi":"10.1002/hem3.70051","DOIUrl":null,"url":null,"abstract":"<p>Allogeneic hematopoietic stem cell transplantation (HSCT) is an important treatment option for high-risk hematologic malignancies that harnesses the graft-versus-leukemia effect and employs a conditioning regimen to eradicate residual leukemic cells.<span><sup>1, 2</sup></span> High-risk acute lymphoblastic leukemia (ALL), including relapsed or refractory cases, remains a major indication for allogeneic HSCT in the pediatric population.<span><sup>1-5</sup></span></p><p>Myeloablative conditioning regimens using total body irradiation (TBI) have demonstrated better outcomes than those of chemoconditioning in various pivotal prospective trials.<span><sup>6-8</sup></span> Most notably, the recently published FORUM trial demonstrated a superior overall survival (OS) rate and lower cumulative incidence (CI) of relapse and treatment-related mortality with 12 Gy TBI plus etoposide compared with those of chemoconditioning with fludarabine, thiotepa, and either busulfan or treosulfan in high-risk pediatric patients with ALL above 4 years of age.<span><sup>8</sup></span> However, there remains an unmet need for chemoconditioning regimens for pediatric patients below 4 years of age. Additionally, concerns persist regarding the long-term complications of TBI with myeloablative dosing, particularly in the pediatric population, such as secondary malignancy and endocrinologic problems.<span><sup>9-11</sup></span></p><p>Busulfan is a key chemotherapeutic drug for chemoconditioning; however, it exhibits variable pharmacokinetic profiles.<span><sup>12</sup></span> To optimize busulfan dosing and reduce unexpected toxicity or underdosing, our institution has implemented intensive pharmacokinetic monitoring of busulfan for chemoconditioning yielding favorable outcomes in HSCT for pediatric leukemia.<span><sup>13, 14</sup></span> In particular, our previous report on a chemoconditioning regimen utilizing targeted busulfan, fludarabine, and etoposide in high-risk pediatric patients with ALL showed promising outcomes.<span><sup>15</sup></span></p><p>Herein, we present the findings of a prospective phase II trial (ClinicalTrials.gov: NCT02047578) evaluating the efficacy of targeted busulfan (the target busulfan area under the curve [AUC] between 74 and 76 mg × h/L), fludarabine (40 mg/m², once daily, 5 days), and etoposide (20 mg/kg, once daily, 3 days) conditioning regimens for allogeneic HSCT using matched sibling or unrelated donors in pediatric patients with high-risk ALL. The primary outcome of this study was the 1-year event-free survival (EFS) rate after HSCT, which was anticipated to exceed 80%. We estimated the sample size as a 20% increase in the 1-year EFS rate (to 80%) compared to historical data, with a type I error of 5% and a power of 80%. This study began in February 2014, and the final patient was enrolled in August 2021. The Institutional Review Board of our institution approved the study protocol (H-1210-066-434), and written informed consent was obtained from the parents of all participating patients. More detailed methods and results can be found in the Supporting Information document.</p><p>A total of 36 patients were included in this study (Table 1). The median age at HSCT was 8.1 years (range, 1.0–18.9), and the median follow-up time post-HSCT was 5.6 years (range, 0.8–10.1). All patients completed the planned conditioning regimen, and there were no early deaths within 3 months post-HSCT. Among the donors, 38.9% were matched sibling donors (MSDs) and 61.1% were matched unrelated donors (MUDs); 47.2% had 10/10 matches and 13.9% had 9/10 matches. All patients received peripheral blood stem cells as the stem cell source. Daily intensive pharmacokinetic monitoring of busulfan targeted a total 4-day AUC between 74 and 76 mg × h/L. The median total busulfan AUC was 74.9 mg × h/L. However, because of unexpected clearance changes, the total busulfan AUC was lower than 74 mg × h/L in 11 patients and higher than 76 mg × h/L in nine patients (Supporting Information S1: Figure S1).</p><p>All patients achieved neutrophil and platelet engraftment (Supporting Information S1: Figure S2). The median time to neutrophil counts above 500/µL and 1000/µL was 10 days (range, 9–12) and 10 days (range, 9–16), respectively. Similarly, the median time to platelet counts above 20 × 10<sup>3</sup>/µL and 50 × 10<sup>3</sup>/µL was 13 days (range, 10–23) and 13 days (range, 10–32), respectively.</p><p>No regimen-related deaths occurred within 42 days after HSCT. Hepatic veno-occlusive disease occurred in three patients, with two cases being classified as severe. The busulfan AUCs of the two patients who demonstrated severe VOD were 73.6 and 76.4 mg × h/L, respectively. CMV reactivation was observed in 20 patients (55.6%), without cases of CMV disease. No cases of posttransplantation lymphoproliferative disease were reported (Supporting Information S1: Table S1). With a median follow-up period of 5.6 years (range, 0.8–10.1), there were no cases of secondary malignancy.</p><p>The CI rates for grades II–IV and III–IV acute graft-versus-host disease (GVHD) were 36.1% and 2.8%, respectively (Figure 1A). The CI rate for chronic GVHD was 17.0%, with a moderate-to-severe rate of 8.4% (Figure 1B). Organs involved in moderate-to-severe chronic GVHD included the skin (100%), mouth (67%), and liver (33%). None of the deaths were associated with GVHD.</p><p>The CI rate for relapse was 33.4% (Figure 1C). Among the 12 patients who experienced relapse, five died owing to disease progression or complications related to salvage chemotherapy, with a median time from relapse of 414 days (range, 147–1056). The remaining seven patients were alive and disease-free at their last follow-up. Among all relapsed patients, seven relapsed within 1-year post-HSCT showing a tendency toward worse 3-year EFS rates (28.6% vs. 75.0%, <i>p</i> = 0.065) and OS rates (42.9% vs. 66.7%, <i>p</i> = 0.200) compared to those who relapsed after 1-year post-HSCT (Figure S3).</p><p>The CI rate for nonrelapse mortality (NRM) was 2.8% (Figure 1C). One patient diagnosed with infant ALL died on day 501 post-HSCT due to sudden respiratory failure following viral pneumonia. The patient had been receiving prolonged prednisolone therapy for Evans syndrome.</p><p>The 5-year moderate-severe chronic GVHD, event-free survival (GEFS), EFS, and OS rates were 55.6% (95% CI: 39.3–71.9), 63.9% (95% CI: 48.2–79.6), and 86.1% (95% CI: 74.7–97.5), respectively (Figure 1D). The 1-year EFS and OS rates were 80.6% (95% CI: 67.7–93.5) and 94.4% (95% CI: 87.0–100.0), respectively, with 2-year rates of 69.4% (95% CI: 54.3–84.5) and 86.1% (95% CI: 74.7–97.5). Notably, a 1-year EFS rate of 80.6% met the primary outcome of the study.</p><p>The survival outcomes for each factor are summarized in Supporting Information S1: Table S2. Although the pediatric disease risk index was associated with worse 5-year EFS rates in the univariate analysis (low 77.3% vs. intermediate 42.9%, <i>p</i> = 0.04), it was not significant in the multivariate analysis. There was no statistically significant prognostic factor in the multivariate analysis; however, a total busulfan AUC < 74 mg × h/L showed a tendency toward worse 5-year EFS rates (hazard ratio: 3.5, <i>p</i> = 0.08).</p><p>Our study demonstrated 5-year EFS and OS rates of 63.9% and 86.1%, respectively, among pediatric and adolescent patients with ALL requiring HSCT. To our knowledge, this is the first prospective study of pediatric patients using the conditioning regimen comprising targeted busulfan, fludarabine, and etoposide without TBI. Optimization of the busulfan AUC through intensive pharmacokinetic monitoring reduced toxicity, resulting in a low NRM rate of 2.8%. Furthermore, over half of the patients who relapsed following HSCT were successfully salvaged through subsequent therapies, leading to prolonged survival.</p><p>However, the superior treatment outcomes of TBI-containing myeloablative conditioning regimens in ALL have been well established, not only in adults but also in pediatric populations through several studies.<span><sup>6-8, 16-18</sup></span> Particularly in the pivotal FORUM trial, lower 2-year treatment-related mortality and relapse incidences with TBI conditioning compared to those with chemoconditioning (2% vs. 9% and 12% vs. 33%, respectively) translated into better EFS and OS.<span><sup>8</sup></span> The EFS rates in our study were similar to those in the chemoconditioning arm of the FORUM trial, but the lower observed toxicity in our study may have contributed to the higher OS rates (86.1% at 5 years compared to 75% reported in the FORUM study).</p><p>Given the long-term toxicity concerns of TBI conditioning, it is imperative to continue employing appropriate chemoconditioning, particularly in children under 4 years of age, where the use of myeloablative doses of TBI is challenging. Recently published outcomes of chemoconditioning HSCT in patients under 4 years of age (utilizing fludarabine, thiotepa, busulfan, or treosulfan) demonstrated a low NRM rate of 3%–6%. However, the relapse rate remained high at 42%–45%, resulting in a 3-year EFS of 52%.<span><sup>19</sup></span> In the current study, only 5 patients under 4 years of age at the time of transplantation were included. Among them, three patients achieved long-term survival, whereas two patients died (one due to relapse and disease progression and one due to NRM). Previously, our institution reported a 1-year OS of 83.3% in infant patients with ALL through retrospective analysis.<span><sup>15</sup></span> The targeted busulfan dosing, guided by intensive pharmacokinetic monitoring, may account for the promising outcomes observed with a lower NRM rate in our study. We observed a trend toward improved GEFS and EFS, as well as significantly better OS among patients who received the target AUC of busulfan in the univariate analysis, although this association was not significant in the multivariate analysis. In our study, we established a target busulfan total AUC of 74–76 mg × h/L. However, due to the highly variable pharmacokinetics of busulfan, this range may be relatively narrow. As a result of fluctuations in clearance, 20 patients (55.6%) did not achieve this target. This indicates that busulfan, when administered without individualized dosing, can lead to significant variability in AUCs. These findings may help explain the improved outcomes observed in our study compared to the results of the FORUM study on busulfan-based chemoconditioning.<span><sup>8</sup></span></p><p>Furthermore, despite its favorable outcomes, TBI conditioning transplantation carries a higher risk of long-term complications, such as secondary malignancies. Notably, with longer-term observations, the 10-year CI of secondary malignancies has been reported to reach up to 13% in groups utilizing TBI compared to 0% in chemoconditioning groups,<span><sup>20</sup></span> underscoring the necessity for long-term follow-up. To our knowledge, no cases of secondary malignancies have been reported to date.</p><p>However, this study has several limitations. First, as it was a single-arm trial, comparing it with other conditioning regimens is challenging. Second, the limited number of patients enrolled at a single institution restricts the generalizability of these results. Nevertheless, given its promising toxicity profile and efficacy, our study presents a viable non-TBI conditioning regimen for pediatric patients with high-risk ALL who are not suitable candidates for myeloablative TBI conditioning, particularly among younger patients.</p><p>In conclusion, this prospective, single-arm, phase II trial demonstrated the feasibility of a non-TBI conditioning regimen comprising targeted busulfan, fludarabine, and etoposide, with lower NRM and promising OS rates. With growing concerns regarding myeloablative TBI, the development of various immunotherapies, and NGS-MRD, further studies are warranted to ascertain the role of myeloablative chemoconditioning in pediatric populations with high-risk ALL.</p><p>Hyoung Jin Kang initiated the project. Kyung Taek Hong, Sang Hoon Song, SeungHwan Lee, Kyung-Sang Yu, In-Jin Jang, and Hyoung Jin Kang participated in the study design and performed the research. Kyung Taek Hong, Hyun Jin Park, Bo Kyung Kim, and Jung Yoon Choi participated in data collection. Kyung Taek Hong participated in statistical analysis/interpretation and wrote the manuscript. Kyung Taek Hong and Hyoung Jin Kang participated in manuscript editing. All authors have read and approved the manuscript.</p><p>The authors declare no conflict of interest.</p><p>This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2022-KH123868).</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 12","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-11-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.70051","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70051","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Allogeneic hematopoietic stem cell transplantation (HSCT) is an important treatment option for high-risk hematologic malignancies that harnesses the graft-versus-leukemia effect and employs a conditioning regimen to eradicate residual leukemic cells.1, 2 High-risk acute lymphoblastic leukemia (ALL), including relapsed or refractory cases, remains a major indication for allogeneic HSCT in the pediatric population.1-5
Myeloablative conditioning regimens using total body irradiation (TBI) have demonstrated better outcomes than those of chemoconditioning in various pivotal prospective trials.6-8 Most notably, the recently published FORUM trial demonstrated a superior overall survival (OS) rate and lower cumulative incidence (CI) of relapse and treatment-related mortality with 12 Gy TBI plus etoposide compared with those of chemoconditioning with fludarabine, thiotepa, and either busulfan or treosulfan in high-risk pediatric patients with ALL above 4 years of age.8 However, there remains an unmet need for chemoconditioning regimens for pediatric patients below 4 years of age. Additionally, concerns persist regarding the long-term complications of TBI with myeloablative dosing, particularly in the pediatric population, such as secondary malignancy and endocrinologic problems.9-11
Busulfan is a key chemotherapeutic drug for chemoconditioning; however, it exhibits variable pharmacokinetic profiles.12 To optimize busulfan dosing and reduce unexpected toxicity or underdosing, our institution has implemented intensive pharmacokinetic monitoring of busulfan for chemoconditioning yielding favorable outcomes in HSCT for pediatric leukemia.13, 14 In particular, our previous report on a chemoconditioning regimen utilizing targeted busulfan, fludarabine, and etoposide in high-risk pediatric patients with ALL showed promising outcomes.15
Herein, we present the findings of a prospective phase II trial (ClinicalTrials.gov: NCT02047578) evaluating the efficacy of targeted busulfan (the target busulfan area under the curve [AUC] between 74 and 76 mg × h/L), fludarabine (40 mg/m², once daily, 5 days), and etoposide (20 mg/kg, once daily, 3 days) conditioning regimens for allogeneic HSCT using matched sibling or unrelated donors in pediatric patients with high-risk ALL. The primary outcome of this study was the 1-year event-free survival (EFS) rate after HSCT, which was anticipated to exceed 80%. We estimated the sample size as a 20% increase in the 1-year EFS rate (to 80%) compared to historical data, with a type I error of 5% and a power of 80%. This study began in February 2014, and the final patient was enrolled in August 2021. The Institutional Review Board of our institution approved the study protocol (H-1210-066-434), and written informed consent was obtained from the parents of all participating patients. More detailed methods and results can be found in the Supporting Information document.
A total of 36 patients were included in this study (Table 1). The median age at HSCT was 8.1 years (range, 1.0–18.9), and the median follow-up time post-HSCT was 5.6 years (range, 0.8–10.1). All patients completed the planned conditioning regimen, and there were no early deaths within 3 months post-HSCT. Among the donors, 38.9% were matched sibling donors (MSDs) and 61.1% were matched unrelated donors (MUDs); 47.2% had 10/10 matches and 13.9% had 9/10 matches. All patients received peripheral blood stem cells as the stem cell source. Daily intensive pharmacokinetic monitoring of busulfan targeted a total 4-day AUC between 74 and 76 mg × h/L. The median total busulfan AUC was 74.9 mg × h/L. However, because of unexpected clearance changes, the total busulfan AUC was lower than 74 mg × h/L in 11 patients and higher than 76 mg × h/L in nine patients (Supporting Information S1: Figure S1).
All patients achieved neutrophil and platelet engraftment (Supporting Information S1: Figure S2). The median time to neutrophil counts above 500/µL and 1000/µL was 10 days (range, 9–12) and 10 days (range, 9–16), respectively. Similarly, the median time to platelet counts above 20 × 103/µL and 50 × 103/µL was 13 days (range, 10–23) and 13 days (range, 10–32), respectively.
No regimen-related deaths occurred within 42 days after HSCT. Hepatic veno-occlusive disease occurred in three patients, with two cases being classified as severe. The busulfan AUCs of the two patients who demonstrated severe VOD were 73.6 and 76.4 mg × h/L, respectively. CMV reactivation was observed in 20 patients (55.6%), without cases of CMV disease. No cases of posttransplantation lymphoproliferative disease were reported (Supporting Information S1: Table S1). With a median follow-up period of 5.6 years (range, 0.8–10.1), there were no cases of secondary malignancy.
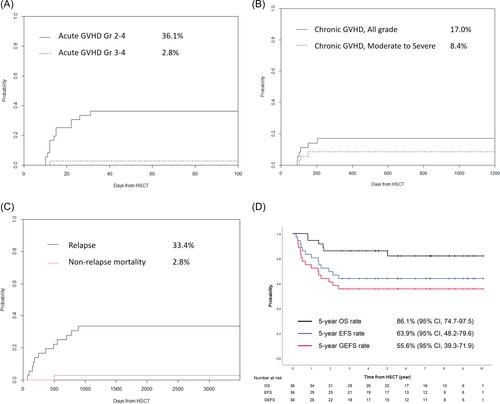
The CI rates for grades II–IV and III–IV acute graft-versus-host disease (GVHD) were 36.1% and 2.8%, respectively (Figure 1A). The CI rate for chronic GVHD was 17.0%, with a moderate-to-severe rate of 8.4% (Figure 1B). Organs involved in moderate-to-severe chronic GVHD included the skin (100%), mouth (67%), and liver (33%). None of the deaths were associated with GVHD.
The CI rate for relapse was 33.4% (Figure 1C). Among the 12 patients who experienced relapse, five died owing to disease progression or complications related to salvage chemotherapy, with a median time from relapse of 414 days (range, 147–1056). The remaining seven patients were alive and disease-free at their last follow-up. Among all relapsed patients, seven relapsed within 1-year post-HSCT showing a tendency toward worse 3-year EFS rates (28.6% vs. 75.0%, p = 0.065) and OS rates (42.9% vs. 66.7%, p = 0.200) compared to those who relapsed after 1-year post-HSCT (Figure S3).
The CI rate for nonrelapse mortality (NRM) was 2.8% (Figure 1C). One patient diagnosed with infant ALL died on day 501 post-HSCT due to sudden respiratory failure following viral pneumonia. The patient had been receiving prolonged prednisolone therapy for Evans syndrome.
The 5-year moderate-severe chronic GVHD, event-free survival (GEFS), EFS, and OS rates were 55.6% (95% CI: 39.3–71.9), 63.9% (95% CI: 48.2–79.6), and 86.1% (95% CI: 74.7–97.5), respectively (Figure 1D). The 1-year EFS and OS rates were 80.6% (95% CI: 67.7–93.5) and 94.4% (95% CI: 87.0–100.0), respectively, with 2-year rates of 69.4% (95% CI: 54.3–84.5) and 86.1% (95% CI: 74.7–97.5). Notably, a 1-year EFS rate of 80.6% met the primary outcome of the study.
The survival outcomes for each factor are summarized in Supporting Information S1: Table S2. Although the pediatric disease risk index was associated with worse 5-year EFS rates in the univariate analysis (low 77.3% vs. intermediate 42.9%, p = 0.04), it was not significant in the multivariate analysis. There was no statistically significant prognostic factor in the multivariate analysis; however, a total busulfan AUC < 74 mg × h/L showed a tendency toward worse 5-year EFS rates (hazard ratio: 3.5, p = 0.08).
Our study demonstrated 5-year EFS and OS rates of 63.9% and 86.1%, respectively, among pediatric and adolescent patients with ALL requiring HSCT. To our knowledge, this is the first prospective study of pediatric patients using the conditioning regimen comprising targeted busulfan, fludarabine, and etoposide without TBI. Optimization of the busulfan AUC through intensive pharmacokinetic monitoring reduced toxicity, resulting in a low NRM rate of 2.8%. Furthermore, over half of the patients who relapsed following HSCT were successfully salvaged through subsequent therapies, leading to prolonged survival.
However, the superior treatment outcomes of TBI-containing myeloablative conditioning regimens in ALL have been well established, not only in adults but also in pediatric populations through several studies.6-8, 16-18 Particularly in the pivotal FORUM trial, lower 2-year treatment-related mortality and relapse incidences with TBI conditioning compared to those with chemoconditioning (2% vs. 9% and 12% vs. 33%, respectively) translated into better EFS and OS.8 The EFS rates in our study were similar to those in the chemoconditioning arm of the FORUM trial, but the lower observed toxicity in our study may have contributed to the higher OS rates (86.1% at 5 years compared to 75% reported in the FORUM study).
Given the long-term toxicity concerns of TBI conditioning, it is imperative to continue employing appropriate chemoconditioning, particularly in children under 4 years of age, where the use of myeloablative doses of TBI is challenging. Recently published outcomes of chemoconditioning HSCT in patients under 4 years of age (utilizing fludarabine, thiotepa, busulfan, or treosulfan) demonstrated a low NRM rate of 3%–6%. However, the relapse rate remained high at 42%–45%, resulting in a 3-year EFS of 52%.19 In the current study, only 5 patients under 4 years of age at the time of transplantation were included. Among them, three patients achieved long-term survival, whereas two patients died (one due to relapse and disease progression and one due to NRM). Previously, our institution reported a 1-year OS of 83.3% in infant patients with ALL through retrospective analysis.15 The targeted busulfan dosing, guided by intensive pharmacokinetic monitoring, may account for the promising outcomes observed with a lower NRM rate in our study. We observed a trend toward improved GEFS and EFS, as well as significantly better OS among patients who received the target AUC of busulfan in the univariate analysis, although this association was not significant in the multivariate analysis. In our study, we established a target busulfan total AUC of 74–76 mg × h/L. However, due to the highly variable pharmacokinetics of busulfan, this range may be relatively narrow. As a result of fluctuations in clearance, 20 patients (55.6%) did not achieve this target. This indicates that busulfan, when administered without individualized dosing, can lead to significant variability in AUCs. These findings may help explain the improved outcomes observed in our study compared to the results of the FORUM study on busulfan-based chemoconditioning.8
Furthermore, despite its favorable outcomes, TBI conditioning transplantation carries a higher risk of long-term complications, such as secondary malignancies. Notably, with longer-term observations, the 10-year CI of secondary malignancies has been reported to reach up to 13% in groups utilizing TBI compared to 0% in chemoconditioning groups,20 underscoring the necessity for long-term follow-up. To our knowledge, no cases of secondary malignancies have been reported to date.
However, this study has several limitations. First, as it was a single-arm trial, comparing it with other conditioning regimens is challenging. Second, the limited number of patients enrolled at a single institution restricts the generalizability of these results. Nevertheless, given its promising toxicity profile and efficacy, our study presents a viable non-TBI conditioning regimen for pediatric patients with high-risk ALL who are not suitable candidates for myeloablative TBI conditioning, particularly among younger patients.
In conclusion, this prospective, single-arm, phase II trial demonstrated the feasibility of a non-TBI conditioning regimen comprising targeted busulfan, fludarabine, and etoposide, with lower NRM and promising OS rates. With growing concerns regarding myeloablative TBI, the development of various immunotherapies, and NGS-MRD, further studies are warranted to ascertain the role of myeloablative chemoconditioning in pediatric populations with high-risk ALL.
Hyoung Jin Kang initiated the project. Kyung Taek Hong, Sang Hoon Song, SeungHwan Lee, Kyung-Sang Yu, In-Jin Jang, and Hyoung Jin Kang participated in the study design and performed the research. Kyung Taek Hong, Hyun Jin Park, Bo Kyung Kim, and Jung Yoon Choi participated in data collection. Kyung Taek Hong participated in statistical analysis/interpretation and wrote the manuscript. Kyung Taek Hong and Hyoung Jin Kang participated in manuscript editing. All authors have read and approved the manuscript.
The authors declare no conflict of interest.
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2022-KH123868).
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
