Kinetics of lymphocytosis in naïve chronic lymphocytic leukemia patients treated with covalent Bruton's tyrosine kinase inhibitors: An Italian multicenter real-life experience
Idanna Innocenti, Antonio Mosca, Annamaria Tomasso, Andrea Galitzia, Lydia Scarfò, Francesca Morelli, Eugenio Galli, Francesca Martini, Eugenio Sangiorgi, Roberta Laureana, Giulia Benintende, Veronica Mattiello, Sabrina Chiriu, Maria I. Del Principe, Giulia Zamprogna, Massimo Gentile, Enrica A. Martino, Emilia Cappello, Maria C. Montalbano, Giuliana Farina, Vanessa Innao, Luca Stirparo, Caterina Patti, Paolo Sportoletti, Alberto Fresa, Gioacchino Catania, Marta Coscia, Silvia Bellesi, Alessandra Tedeschi, Alessandro Sanna, Andrea Visentin, Francesco Autore, Raffaella Pasquale, Livio Trentin, Marzia Varettoni, Paolo Ghia, Roberta Murru, Luca Laurenti
{"title":"Kinetics of lymphocytosis in naïve chronic lymphocytic leukemia patients treated with covalent Bruton's tyrosine kinase inhibitors: An Italian multicenter real-life experience","authors":"Idanna Innocenti, Antonio Mosca, Annamaria Tomasso, Andrea Galitzia, Lydia Scarfò, Francesca Morelli, Eugenio Galli, Francesca Martini, Eugenio Sangiorgi, Roberta Laureana, Giulia Benintende, Veronica Mattiello, Sabrina Chiriu, Maria I. Del Principe, Giulia Zamprogna, Massimo Gentile, Enrica A. Martino, Emilia Cappello, Maria C. Montalbano, Giuliana Farina, Vanessa Innao, Luca Stirparo, Caterina Patti, Paolo Sportoletti, Alberto Fresa, Gioacchino Catania, Marta Coscia, Silvia Bellesi, Alessandra Tedeschi, Alessandro Sanna, Andrea Visentin, Francesco Autore, Raffaella Pasquale, Livio Trentin, Marzia Varettoni, Paolo Ghia, Roberta Murru, Luca Laurenti","doi":"10.1002/hem3.144","DOIUrl":null,"url":null,"abstract":"<p>Chronic lymphocytic leukemia (CLL) therapy has recently undergone a revolution with the introduction of a new class of drugs: covalent Bruton's tyrosine kinase inhibitors (cBTKi), paving the way for a chemotherapy-free approach.<span><sup>1-4</sup></span> Presently, cBTKi can be utilized in the first line of CLL management, thanks to the results of phase III clinical trials such as RESONATE-2 and ELEVATE-TN, which demonstrated the superiority of Ibrutinib over chemotherapy with chlorambucil<span><sup>5</sup></span> and acalabrutinib over chemoimmunotherapy with chlorambucil + obinutuzumab,<span><sup>6</sup></span> in terms of progression-free survival (PFS) in both cases. Ibrutinib exhibited better PFS, overall survival (OS), and overall response rate than the monoclonal anti-CD20 antibody ofatumumab in previously treated patients with CLL.<span><sup>7</sup></span> Additionally, the ASCEND study, another phase III randomized clinical trial, demonstrated that acalabrutinib significantly improved PFS compared to a physician's choice of Idelalisib + rituximab or bendamustine + rituximab, in patients with relapsed/refractory CLL.<span><sup>8</sup></span></p><p>BTK plays a pivotal role in B-cell receptor (BCR) signal transduction,<span><sup>9</sup></span> stimulating important pathways such as NFKB<span><sup>10, 11</sup></span> and CXCR4.<span><sup>12</sup></span> Consequently, BTK is involved in B-cell survival, proliferation, and adhesion, while its activation promotes B-cell proliferation.<span><sup>13</sup></span> Paradoxically, ibrutinib has shown to increase absolute lymphocyte count (ALC) in the initial phase of treatment, regardless of previous lines of therapy. Ibrutinib-induced lymphocytosis may be explained by the redistribution of lymphocytes from neoplastic nodal compartments into the peripheral blood.<span><sup>14</sup></span> Furthermore, it was noted that Ibrutinib-induced lymphocytosis is transient in most patients, resolving within 8 months, but may rarely persist for over 12 months without impacting survival.<span><sup>14</sup></span> This evidence led to the introduction of a new criterion in the assessment of CLL therapy response: partial response with lymphocytosis (PR-L).<span><sup>15</sup></span> Subsequently, the kinetics of lymphocytosis in CLL treated with ibrutinib monotherapy showed that lymphocytosis occurred in the majority of patients treated in first line was higher in immunoglobulin variable heavy chain (IGHV) mutated settings and resolved in 95% of patients after a median of 18.4 months.<span><sup>16</sup></span></p><p>Little is known about frequency and duration of lymphocytosis in patients treated with the second-generation cBTKi acalabrutinib. Therefore, the aim of this study is to outline the kinetics of lymphocytosis in CLL patients treated with acalabrutinib compared to ibrutinib.</p><p>We conducted a multicenter retrospective real-life study involving 17 Italian centers. The study was carried out according to the Helsinki Declaration, Good Clinical Practice, and the applicable national regulations and approved by the local ethical committee. All patients provided written informed consent. The primary endpoint was to define the kinetics of lymphocytosis in naïve patients treated with acalabrutinib monotherapy compared to those treated with ibrutinib, over a 12-month observational period. We included patients receiving therapy with ibrutinib or acalabrutinib, in the first line at the target dose of 420 mg/day for ibrutinib and 200 mg/day for acalabrutinib.</p><p>We enrolled 204 patients divided into two arms: the ibrutinib arm (<i>n</i> = 136) and the acalabrutinib arm (<i>n</i> = 68). The median age was 73 years for the ibrutinib arm and 71 for the acalabrutinib arm. For each patient, we defined the clinical and biological features of disease at baseline, including IGHV mutational status, chromosomal abnormalities by FISH, and molecular biology mutations. At baseline, we considered stage, lymph node involvement, and the presence of splenomegaly. Clinical characteristics and molecular features are reported in Table 1.</p><p>Subsequently, we assessed the ALC through serial blood count tests at baseline and at different time points: 2 weeks, 1 month, 2 months, 3 months, 6 months, 9 months, and 12 months after the start of treatment. We calculated the median ALC, expressed both in terms of cells/mm<sup>3</sup> and as a percentage compared to the baseline, at each time point. For statistical analysis, we used the Mann–Whitney test to compare median ALC values, considering only those with a <i>p</i>-value < 0.05 as statistically significant.</p><p>We observed that in the ibrutinib group (IBR), the median ALC at baseline was 63,270/mm<sup>3</sup>, while in the acalabrutinib group (ACALA), it was 82,905/mm<sup>3</sup>. Median ALC peaked at two weeks in both arms and then immediately began to decline, reaching the baseline level at 1 month. From Month 1 to Month 12 ALC steadily declined, reaching a normal lymphocyte count (<4000/mm<sup>3</sup>, according to iwCLL guidelines) at Month 12 for ACALA. ACALA exhibited lower ALC from Month 6 to Month 12 compared to IBR. At Month 12, IBR did not reach the median normal lymphocyte count. For each data point, we calculated the percentage compared to the baseline, which provides a more representative view of lymphocyte count changes at each time point of the study (Supporting Information S1: Table S1).</p><p>Subsequently, we examined the decline in lymphocytosis to understand if well-defined clinical or biological features could independently impact the kinetics of lymphocyte count in both arms. ACALA had less patients with a molecularly unfavorable prognostic profile; despite this, it seems to have no impact on the kinetics of lymphocytosis in both arms according to our subanalysis (data not shown). IGHV mutational status did not differ between the two arms, but IGHV mutational status had an impact on the lymphocytosis decline. We considered separately cases with unmutated and mutated IGHV genes for IBR and ACALA. They exhibited a similar increment at Day 14 followed by a steady decline. Unmutated IGHV curves of IBR and ACALA overlapped until Month 12. Mutated IGHV for IBR and ACALA followed a similar pattern until Month 6, after which ACALA exhibited a stronger reduction, albeit only as a percentage of baseline, due to ACALA starting from a higher baseline level (Figure 1, Supporting Information S1: Tables S2 and S3). Because there were more cases with TP53 mutations (del17p or TP53 mutated), we evaluated whether the TP53 mutational status had an impact on ALC kinetics within the subgroups. As shown in Supporting Information S1: Table S4, there was no difference in ALC kinetics according to TP53 mutational status among the IGHV mutated and unmutated cases in the IBR arm.</p><p>Regarding clinical features and the burden of disease at baseline, the two arms were homogeneous with only one exception: more patients treated with acalabrutinib (53%) had Binet staging C before therapy, while only (39%) of patients treated with ibrutinib had stage C. Despite this difference being statistically significant (<i>p</i> = 0.04), our analysis demonstrated that the stage had no impact on the kinetics of lymphocytosis (data not shown). Even with different grades of lymphadenopathy and splenomegaly, including the presence of bulky masses, the trend of lymphocytosis during treatment with both cBTKi remained unaltered (data not shown).</p><p>We have provided the first description of the kinetics of lymphocytosis in patients treated with acalabrutinib and conducted the first comparative study of lymphocyte counts during 12 months of treatment with two cBTK inhibitors. We observed that, similar to Ibrutinib, acalabrutinib leads to an increase in lymphocyte count immediately after starting therapy. This observation confirms previous works identifying lymphocytosis as a “class effect” of cBTKi.<span><sup>14</sup></span></p><p>We observed that while there is an appreciable reduction in lymphocyte count starting from the second month of treatment in both groups, the decrease in lymphocytosis appears to be faster and more profound in patients treated with acalabrutinib from the 6th month onward.</p><p>We also investigated whether certain disease's features could explain the differences in the kinetics of lymphocytosis. There was a significant difference in the distribution of patients with a poor molecular prognosis (del17p/<i>TP53</i>) between the two groups, with a marked prevalence in the IBR arm. This difference can be attributed to the evolution of cBTKi use in clinical practice: when ibrutinib was introduced, it was only allowed for patients with a poor prognosis. Conversely, acalabrutinib was used in clinical practice when the administration of cBTKi was already well established in all untreated patients. However, according to our data, having a del17p/<i>TP53</i> mutation or <i>NOTCH1</i> mutation does not interfere with the kinetics of lymphocytosis during treatment with the two different cBTKi. <i>NOTCH1</i> mutations and higher CD49D expression have been associated with reduced ibrutinib-induced lymphocytosis,<span><sup>17, 18</sup></span> but in this cohort, we did not observe any effect. The IGHV mutational status did not differ between the two groups; however, when examining lymphocyte count curves in mutated IGHV, starting from the 6th month to the end of the study period, the median percentage of baseline declined more in the ACALA arm reaching a statistical difference. Overall, IGHV mutated/unmutated patients treated with acalabrutinib had a similar increase in lymphocyte count after 14 days, followed by a sharper decline, achieving median normal lymphocyte count earlier than the IBR arm. These data suggest that the main differences of lymphocytes count between the two cBTKi is due to IGHV mutated status. The clinical burden of disease at baseline had no impact on the kinetics of lymphocytosis between the two arms.</p><p>Currently, there is lack of data in the literature comparing the differences between ACALA and IBR concerning lymphocytosis, IGHV mutational status, and the extent of lymphocyte mobilization in peripheral blood. Particularly, there is scarcity of mechanistic explanations for the divergent behavior of the two cBTK inhibitors. In order to verify this hypothesis, our group is conducting research into chemokine receptors and adhesion molecules.</p><p>In conclusion, we describe the kinetics of peripheral blood lymphocytosis after ibrutinib or acalabrutinib in patients with CLL treated in front line. Both treatments exhibited a similar peak at 2 weeks after initiation, followed by a more pronounced and rapid decrease in the acalabrutinib treatment group, particularly in IGHV mutated cases.</p><p>Antonio Mosca, Annamaria Tomasso, Andrea Galitzia, Luca Stirparo, Francesca Martini, Francesca Morelli, Roberta Laureana, Giulia Benintende, Veronica Mattiello, Sabrina Chiriu, Maria I. Del Principe, Giulia Zamprogna, Massimo Gentile, Enrica A. Martino, Emilia Cappello, Maria C. Montalbano, Giuliana Farina, Vanessa Innao, Lydia Scarfò, Caterina Patti, Paolo Sportoletti, Alberto Fresa, Gioacchino Catania, Marta Coscia, Silvia Bellesi, Alessandra Tedeschi, Alessandro Sanna, Andrea Visentin, Francesco Autore, Raffaella Pasquale, Livio Trentin, Marzia Varettoni, Paolo Ghia, and Roberta Murru collected the data. Eugenio Galli performed the statistical analysis. Idanna Innocenti and Antonio Mosca wrote the manuscript and Eugenio Sangiorgi and Luca Laurenti supervised the project.</p><p>Paolo Ghia received honoraria from AbbVie, AstraZeneca, BeiGene, BMS, Galapagos, Janssen, Lilly/LoxoOncology, MSD, and Roche, and research funding from AbbVie, AstraZeneca, BMS, and Janssen, and is an Editor of HemaSphere. Marzia Varettoni received honoraria from AbbVie, AstraZeneca, BeiGene, and Janssen. The remaining authors declare no conflict of interest.</p><p>This research received no external funding.</p><p>This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Fondazione Policlinico Universitario Agostino Gemelli IRCCS (Prot. ID 5765 13/10/2023). Written informed consent was obtained from the patients to publish this study.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 12","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-11-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.144","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.144","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Chronic lymphocytic leukemia (CLL) therapy has recently undergone a revolution with the introduction of a new class of drugs: covalent Bruton's tyrosine kinase inhibitors (cBTKi), paving the way for a chemotherapy-free approach.1-4 Presently, cBTKi can be utilized in the first line of CLL management, thanks to the results of phase III clinical trials such as RESONATE-2 and ELEVATE-TN, which demonstrated the superiority of Ibrutinib over chemotherapy with chlorambucil5 and acalabrutinib over chemoimmunotherapy with chlorambucil + obinutuzumab,6 in terms of progression-free survival (PFS) in both cases. Ibrutinib exhibited better PFS, overall survival (OS), and overall response rate than the monoclonal anti-CD20 antibody ofatumumab in previously treated patients with CLL.7 Additionally, the ASCEND study, another phase III randomized clinical trial, demonstrated that acalabrutinib significantly improved PFS compared to a physician's choice of Idelalisib + rituximab or bendamustine + rituximab, in patients with relapsed/refractory CLL.8
BTK plays a pivotal role in B-cell receptor (BCR) signal transduction,9 stimulating important pathways such as NFKB10, 11 and CXCR4.12 Consequently, BTK is involved in B-cell survival, proliferation, and adhesion, while its activation promotes B-cell proliferation.13 Paradoxically, ibrutinib has shown to increase absolute lymphocyte count (ALC) in the initial phase of treatment, regardless of previous lines of therapy. Ibrutinib-induced lymphocytosis may be explained by the redistribution of lymphocytes from neoplastic nodal compartments into the peripheral blood.14 Furthermore, it was noted that Ibrutinib-induced lymphocytosis is transient in most patients, resolving within 8 months, but may rarely persist for over 12 months without impacting survival.14 This evidence led to the introduction of a new criterion in the assessment of CLL therapy response: partial response with lymphocytosis (PR-L).15 Subsequently, the kinetics of lymphocytosis in CLL treated with ibrutinib monotherapy showed that lymphocytosis occurred in the majority of patients treated in first line was higher in immunoglobulin variable heavy chain (IGHV) mutated settings and resolved in 95% of patients after a median of 18.4 months.16
Little is known about frequency and duration of lymphocytosis in patients treated with the second-generation cBTKi acalabrutinib. Therefore, the aim of this study is to outline the kinetics of lymphocytosis in CLL patients treated with acalabrutinib compared to ibrutinib.
We conducted a multicenter retrospective real-life study involving 17 Italian centers. The study was carried out according to the Helsinki Declaration, Good Clinical Practice, and the applicable national regulations and approved by the local ethical committee. All patients provided written informed consent. The primary endpoint was to define the kinetics of lymphocytosis in naïve patients treated with acalabrutinib monotherapy compared to those treated with ibrutinib, over a 12-month observational period. We included patients receiving therapy with ibrutinib or acalabrutinib, in the first line at the target dose of 420 mg/day for ibrutinib and 200 mg/day for acalabrutinib.
We enrolled 204 patients divided into two arms: the ibrutinib arm (n = 136) and the acalabrutinib arm (n = 68). The median age was 73 years for the ibrutinib arm and 71 for the acalabrutinib arm. For each patient, we defined the clinical and biological features of disease at baseline, including IGHV mutational status, chromosomal abnormalities by FISH, and molecular biology mutations. At baseline, we considered stage, lymph node involvement, and the presence of splenomegaly. Clinical characteristics and molecular features are reported in Table 1.
Subsequently, we assessed the ALC through serial blood count tests at baseline and at different time points: 2 weeks, 1 month, 2 months, 3 months, 6 months, 9 months, and 12 months after the start of treatment. We calculated the median ALC, expressed both in terms of cells/mm3 and as a percentage compared to the baseline, at each time point. For statistical analysis, we used the Mann–Whitney test to compare median ALC values, considering only those with a p-value < 0.05 as statistically significant.
We observed that in the ibrutinib group (IBR), the median ALC at baseline was 63,270/mm3, while in the acalabrutinib group (ACALA), it was 82,905/mm3. Median ALC peaked at two weeks in both arms and then immediately began to decline, reaching the baseline level at 1 month. From Month 1 to Month 12 ALC steadily declined, reaching a normal lymphocyte count (<4000/mm3, according to iwCLL guidelines) at Month 12 for ACALA. ACALA exhibited lower ALC from Month 6 to Month 12 compared to IBR. At Month 12, IBR did not reach the median normal lymphocyte count. For each data point, we calculated the percentage compared to the baseline, which provides a more representative view of lymphocyte count changes at each time point of the study (Supporting Information S1: Table S1).
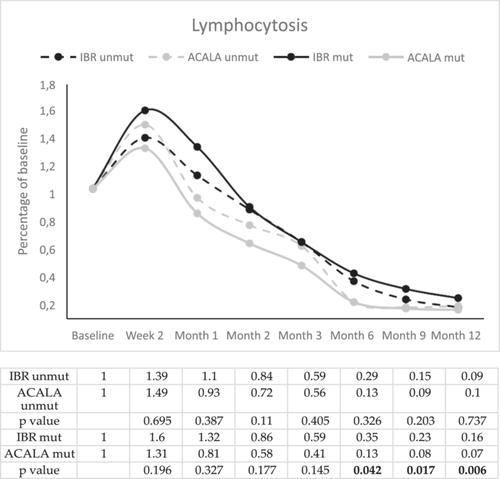
Subsequently, we examined the decline in lymphocytosis to understand if well-defined clinical or biological features could independently impact the kinetics of lymphocyte count in both arms. ACALA had less patients with a molecularly unfavorable prognostic profile; despite this, it seems to have no impact on the kinetics of lymphocytosis in both arms according to our subanalysis (data not shown). IGHV mutational status did not differ between the two arms, but IGHV mutational status had an impact on the lymphocytosis decline. We considered separately cases with unmutated and mutated IGHV genes for IBR and ACALA. They exhibited a similar increment at Day 14 followed by a steady decline. Unmutated IGHV curves of IBR and ACALA overlapped until Month 12. Mutated IGHV for IBR and ACALA followed a similar pattern until Month 6, after which ACALA exhibited a stronger reduction, albeit only as a percentage of baseline, due to ACALA starting from a higher baseline level (Figure 1, Supporting Information S1: Tables S2 and S3). Because there were more cases with TP53 mutations (del17p or TP53 mutated), we evaluated whether the TP53 mutational status had an impact on ALC kinetics within the subgroups. As shown in Supporting Information S1: Table S4, there was no difference in ALC kinetics according to TP53 mutational status among the IGHV mutated and unmutated cases in the IBR arm.
Regarding clinical features and the burden of disease at baseline, the two arms were homogeneous with only one exception: more patients treated with acalabrutinib (53%) had Binet staging C before therapy, while only (39%) of patients treated with ibrutinib had stage C. Despite this difference being statistically significant (p = 0.04), our analysis demonstrated that the stage had no impact on the kinetics of lymphocytosis (data not shown). Even with different grades of lymphadenopathy and splenomegaly, including the presence of bulky masses, the trend of lymphocytosis during treatment with both cBTKi remained unaltered (data not shown).
We have provided the first description of the kinetics of lymphocytosis in patients treated with acalabrutinib and conducted the first comparative study of lymphocyte counts during 12 months of treatment with two cBTK inhibitors. We observed that, similar to Ibrutinib, acalabrutinib leads to an increase in lymphocyte count immediately after starting therapy. This observation confirms previous works identifying lymphocytosis as a “class effect” of cBTKi.14
We observed that while there is an appreciable reduction in lymphocyte count starting from the second month of treatment in both groups, the decrease in lymphocytosis appears to be faster and more profound in patients treated with acalabrutinib from the 6th month onward.
We also investigated whether certain disease's features could explain the differences in the kinetics of lymphocytosis. There was a significant difference in the distribution of patients with a poor molecular prognosis (del17p/TP53) between the two groups, with a marked prevalence in the IBR arm. This difference can be attributed to the evolution of cBTKi use in clinical practice: when ibrutinib was introduced, it was only allowed for patients with a poor prognosis. Conversely, acalabrutinib was used in clinical practice when the administration of cBTKi was already well established in all untreated patients. However, according to our data, having a del17p/TP53 mutation or NOTCH1 mutation does not interfere with the kinetics of lymphocytosis during treatment with the two different cBTKi. NOTCH1 mutations and higher CD49D expression have been associated with reduced ibrutinib-induced lymphocytosis,17, 18 but in this cohort, we did not observe any effect. The IGHV mutational status did not differ between the two groups; however, when examining lymphocyte count curves in mutated IGHV, starting from the 6th month to the end of the study period, the median percentage of baseline declined more in the ACALA arm reaching a statistical difference. Overall, IGHV mutated/unmutated patients treated with acalabrutinib had a similar increase in lymphocyte count after 14 days, followed by a sharper decline, achieving median normal lymphocyte count earlier than the IBR arm. These data suggest that the main differences of lymphocytes count between the two cBTKi is due to IGHV mutated status. The clinical burden of disease at baseline had no impact on the kinetics of lymphocytosis between the two arms.
Currently, there is lack of data in the literature comparing the differences between ACALA and IBR concerning lymphocytosis, IGHV mutational status, and the extent of lymphocyte mobilization in peripheral blood. Particularly, there is scarcity of mechanistic explanations for the divergent behavior of the two cBTK inhibitors. In order to verify this hypothesis, our group is conducting research into chemokine receptors and adhesion molecules.
In conclusion, we describe the kinetics of peripheral blood lymphocytosis after ibrutinib or acalabrutinib in patients with CLL treated in front line. Both treatments exhibited a similar peak at 2 weeks after initiation, followed by a more pronounced and rapid decrease in the acalabrutinib treatment group, particularly in IGHV mutated cases.
Antonio Mosca, Annamaria Tomasso, Andrea Galitzia, Luca Stirparo, Francesca Martini, Francesca Morelli, Roberta Laureana, Giulia Benintende, Veronica Mattiello, Sabrina Chiriu, Maria I. Del Principe, Giulia Zamprogna, Massimo Gentile, Enrica A. Martino, Emilia Cappello, Maria C. Montalbano, Giuliana Farina, Vanessa Innao, Lydia Scarfò, Caterina Patti, Paolo Sportoletti, Alberto Fresa, Gioacchino Catania, Marta Coscia, Silvia Bellesi, Alessandra Tedeschi, Alessandro Sanna, Andrea Visentin, Francesco Autore, Raffaella Pasquale, Livio Trentin, Marzia Varettoni, Paolo Ghia, and Roberta Murru collected the data. Eugenio Galli performed the statistical analysis. Idanna Innocenti and Antonio Mosca wrote the manuscript and Eugenio Sangiorgi and Luca Laurenti supervised the project.
Paolo Ghia received honoraria from AbbVie, AstraZeneca, BeiGene, BMS, Galapagos, Janssen, Lilly/LoxoOncology, MSD, and Roche, and research funding from AbbVie, AstraZeneca, BMS, and Janssen, and is an Editor of HemaSphere. Marzia Varettoni received honoraria from AbbVie, AstraZeneca, BeiGene, and Janssen. The remaining authors declare no conflict of interest.
This research received no external funding.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Fondazione Policlinico Universitario Agostino Gemelli IRCCS (Prot. ID 5765 13/10/2023). Written informed consent was obtained from the patients to publish this study.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
