Radhika Pradip Tampi, Duoquan Wang, Salim Abdulla, Muhidin Kassim Mahende, Tegemeo Gavana, Hajirani M Msuya, Augustine Kuwawenaruwa, Michael Mihayo, Felix Brown, Honorati Masanja, Wilbald Anthony, Katia Bruxvoort, Fadhila Kihwele, Godlove Chila, Wei Chang, Marcia Castro, Xiao Ning, Prosper P Chaki, Yeromin P Mlacha, Jessica Cohen, Nicolas A Menzies
{"title":"The 1,7-malaria reactive community-based testing and response (1,7-mRCTR) approach in Tanzania: a cost-effectiveness analysis.","authors":"Radhika Pradip Tampi, Duoquan Wang, Salim Abdulla, Muhidin Kassim Mahende, Tegemeo Gavana, Hajirani M Msuya, Augustine Kuwawenaruwa, Michael Mihayo, Felix Brown, Honorati Masanja, Wilbald Anthony, Katia Bruxvoort, Fadhila Kihwele, Godlove Chila, Wei Chang, Marcia Castro, Xiao Ning, Prosper P Chaki, Yeromin P Mlacha, Jessica Cohen, Nicolas A Menzies","doi":"10.1186/s40249-024-01261-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reactive case detection (RACD) for malaria control has been found effective in low transmission settings, but its impact and cost-effectiveness in moderate-to-high transmission settings are unknown. We conducted an economic evaluation alongside an empirical trial of a modified RACD strategy (1,7-mRCTR) in three moderate-to-high malaria transmission districts in Tanzania.</p><p><strong>Methods: </strong>The costs and cost savings associated with the intervention relative to passive case detection alone were estimated in the study sites of Kilwa, Kibiti, and Rufiji districts in Tanzania from 2019-2021. Empirical cost data were collected using household surveys. The incremental costs of the intervention were calculated from under a societal perspective. Costs are reported in 2022 US dollars. Trial data and malaria registers from health facilities were used to calculate the number of malaria cases detected. We simulated unobserved and distal health effects of the intervention to assess cost-effectiveness in terms of incremental cost-effectiveness ratios (ICERs). Propagated uncertainty was assessed via second-order Monte Carlo simulation, including bootstrapping of empirical data distributions. Incremental costs per disability-adjusted life year (DALY) averted were compared to a willingness-to-pay threshold based on estimated opportunity costs of healthcare spending in Tanzania.</p><p><strong>Results: </strong>The programmatic cost of the 1,7-mRCTR intervention was 5327 United States Dollars (USD) per 1000 population. The combination of reactive and passive case detection in the intervention arm resulted in an additional 445 malaria cases detected per 1000 compared to passive detection alone, yielding an incremental cost per additional case detected of 12.0 USD. Based on modelling results, for every percentage point decline in malaria prevalence, the intervention averted 95.2 cases and 0.04 deaths per 1000 population. On average, the 1,7-mRCTR intervention averted 19.1 DALYs per 1000 population. Compared to passive malaria detection, the ICERs for the 1,7-mRCTR intervention were 7.3 USD per case averted, 16,884 USD per death averted, and 163 USD per DALY averted.</p><p><strong>Conclusions: </strong>Our analysis demonstrates that the 1,7-mRCTR intervention appears to be cost-effective under a willingness-to-pay threshold of 417 USD per DALY averted, showing that modified RACD strategies can provide value for money in moderate-to-high transmission settings.</p>","PeriodicalId":48820,"journal":{"name":"Infectious Diseases of Poverty","volume":"13 1","pages":"92"},"PeriodicalIF":5.5000,"publicationDate":"2024-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11619255/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases of Poverty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40249-024-01261-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Reactive case detection (RACD) for malaria control has been found effective in low transmission settings, but its impact and cost-effectiveness in moderate-to-high transmission settings are unknown. We conducted an economic evaluation alongside an empirical trial of a modified RACD strategy (1,7-mRCTR) in three moderate-to-high malaria transmission districts in Tanzania.
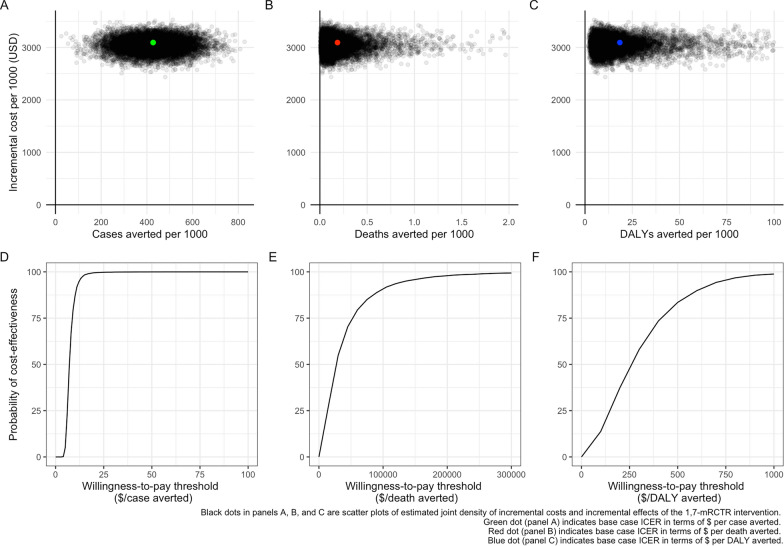
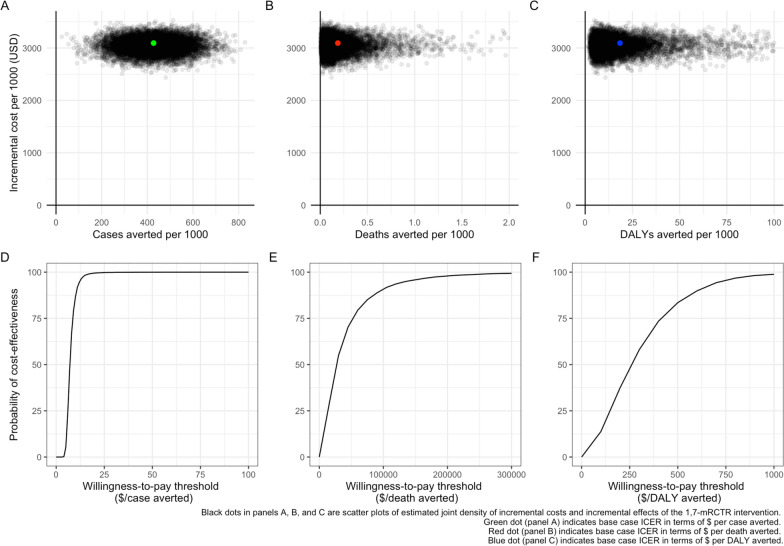
Methods: The costs and cost savings associated with the intervention relative to passive case detection alone were estimated in the study sites of Kilwa, Kibiti, and Rufiji districts in Tanzania from 2019-2021. Empirical cost data were collected using household surveys. The incremental costs of the intervention were calculated from under a societal perspective. Costs are reported in 2022 US dollars. Trial data and malaria registers from health facilities were used to calculate the number of malaria cases detected. We simulated unobserved and distal health effects of the intervention to assess cost-effectiveness in terms of incremental cost-effectiveness ratios (ICERs). Propagated uncertainty was assessed via second-order Monte Carlo simulation, including bootstrapping of empirical data distributions. Incremental costs per disability-adjusted life year (DALY) averted were compared to a willingness-to-pay threshold based on estimated opportunity costs of healthcare spending in Tanzania.
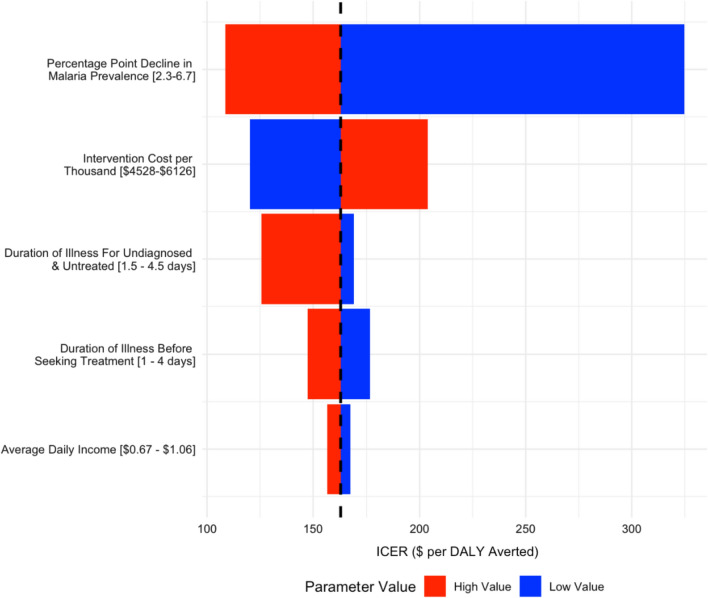
Results: The programmatic cost of the 1,7-mRCTR intervention was 5327 United States Dollars (USD) per 1000 population. The combination of reactive and passive case detection in the intervention arm resulted in an additional 445 malaria cases detected per 1000 compared to passive detection alone, yielding an incremental cost per additional case detected of 12.0 USD. Based on modelling results, for every percentage point decline in malaria prevalence, the intervention averted 95.2 cases and 0.04 deaths per 1000 population. On average, the 1,7-mRCTR intervention averted 19.1 DALYs per 1000 population. Compared to passive malaria detection, the ICERs for the 1,7-mRCTR intervention were 7.3 USD per case averted, 16,884 USD per death averted, and 163 USD per DALY averted.
Conclusions: Our analysis demonstrates that the 1,7-mRCTR intervention appears to be cost-effective under a willingness-to-pay threshold of 417 USD per DALY averted, showing that modified RACD strategies can provide value for money in moderate-to-high transmission settings.
期刊介绍:
Infectious Diseases of Poverty is an open access, peer-reviewed journal that focuses on addressing essential public health questions related to infectious diseases of poverty. The journal covers a wide range of topics including the biology of pathogens and vectors, diagnosis and detection, treatment and case management, epidemiology and modeling, zoonotic hosts and animal reservoirs, control strategies and implementation, new technologies and application. It also considers the transdisciplinary or multisectoral effects on health systems, ecohealth, environmental management, and innovative technology. The journal aims to identify and assess research and information gaps that hinder progress towards new interventions for public health problems in the developing world. Additionally, it provides a platform for discussing these issues to advance research and evidence building for improved public health interventions in poor settings.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
