Developing a thoracoabdominal normothermic regional perfusion (TA-NRP) program for the recovery of organs for thoracic transplant: lessons from the United States experience.
Kyle S Bilodeau, Sarah Y Park, Elizabeth Bashian, Jason Zakko, Michael T Cain, Jessica Y Rove, T Brett Reece, Joseph C Cleveland, Jordan R H Hoffman
{"title":"Developing a thoracoabdominal normothermic regional perfusion (TA-NRP) program for the recovery of organs for thoracic transplant: lessons from the United States experience.","authors":"Kyle S Bilodeau, Sarah Y Park, Elizabeth Bashian, Jason Zakko, Michael T Cain, Jessica Y Rove, T Brett Reece, Joseph C Cleveland, Jordan R H Hoffman","doi":"10.21037/acs-2024-dcd-0038","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Heart and lung transplantation remain efficacious treatments for patients with end-stage cardiopulmonary failure. However, donor shortages remain a challenge to both providers and patients. Thoracoabdominal normothermic regional perfusion (TA-NRP) has been increasingly adopted to decrease organ ischemia from circulatory death donors and therefore increase the number of organs available for transplantation. Despite initial success, data on program genesis and implementation are limited. The aim of this manuscript is to characterize essential human resources, lessons, and key considerations needed to improve TA-NRP dissemination and thus adoption.</p><p><strong>Methods: </strong>Single-center evaluation of a TA-NRP program was conducted using a retrospective cohort study design. All procurements performed using TA-NRP were included. Quantitative data were summarized. Descriptive elements of programmatic genesis, implementation, and experience were summarized using an inductive reasoning approach.</p><p><strong>Results: </strong>Thirty TA-NRP procurements were performed. The average time from incision to TA-NRP initiation was 7±2 minutes and total time on TA-NRP was 87±28 minutes. In simple regression analysis, the average total TA-NRP time was noted to increase by approximately 0.86 minutes per procurement [95% confidence interval (CI): -0.10, 1.82, P=0.08], while the average warm ischemia time was noted to decrease by approximately 0.03 minutes per procurement (95% CI: -0.13, 0.07, P=0.43). Key programmatic elements during planning and implementation were identification of key stakeholders, early communication, proactive navigation of ethical concerns, staffing and equipment needs, and development of TA-NRP algorithms for pre, intra- and post-donation phases of care.</p><p><strong>Conclusions: </strong>Development of a TA-NRP program is both feasible and easily implemented at institutions with pre-existing organ donation after circulatory death (DCD) procurement experience. Early identification of key stakeholders with frequent communication identified areas in need of expanded resources and addressed early ethical concerns, while local implementation efforts supported operationalization of existing infrastructure for TA-NRP procurements.</p>","PeriodicalId":8067,"journal":{"name":"Annals of cardiothoracic surgery","volume":"13 6","pages":"487-494"},"PeriodicalIF":3.1000,"publicationDate":"2024-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11618124/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of cardiothoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/acs-2024-dcd-0038","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Heart and lung transplantation remain efficacious treatments for patients with end-stage cardiopulmonary failure. However, donor shortages remain a challenge to both providers and patients. Thoracoabdominal normothermic regional perfusion (TA-NRP) has been increasingly adopted to decrease organ ischemia from circulatory death donors and therefore increase the number of organs available for transplantation. Despite initial success, data on program genesis and implementation are limited. The aim of this manuscript is to characterize essential human resources, lessons, and key considerations needed to improve TA-NRP dissemination and thus adoption.
Methods: Single-center evaluation of a TA-NRP program was conducted using a retrospective cohort study design. All procurements performed using TA-NRP were included. Quantitative data were summarized. Descriptive elements of programmatic genesis, implementation, and experience were summarized using an inductive reasoning approach.
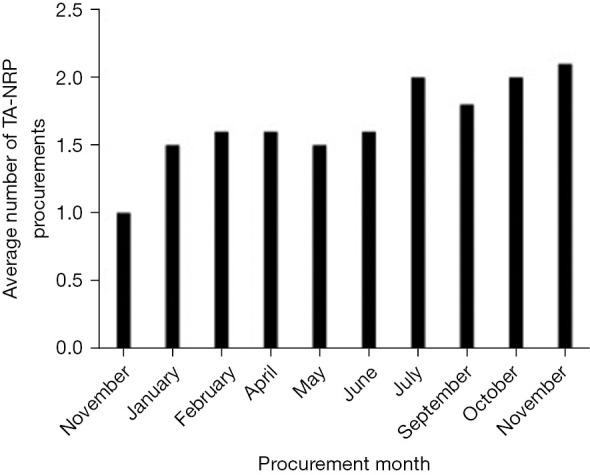
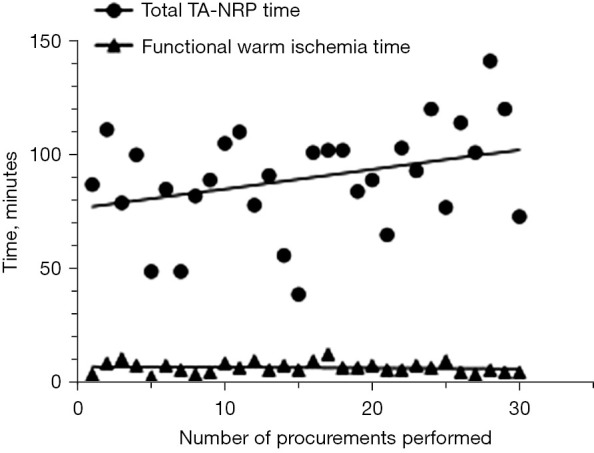
Results: Thirty TA-NRP procurements were performed. The average time from incision to TA-NRP initiation was 7±2 minutes and total time on TA-NRP was 87±28 minutes. In simple regression analysis, the average total TA-NRP time was noted to increase by approximately 0.86 minutes per procurement [95% confidence interval (CI): -0.10, 1.82, P=0.08], while the average warm ischemia time was noted to decrease by approximately 0.03 minutes per procurement (95% CI: -0.13, 0.07, P=0.43). Key programmatic elements during planning and implementation were identification of key stakeholders, early communication, proactive navigation of ethical concerns, staffing and equipment needs, and development of TA-NRP algorithms for pre, intra- and post-donation phases of care.
Conclusions: Development of a TA-NRP program is both feasible and easily implemented at institutions with pre-existing organ donation after circulatory death (DCD) procurement experience. Early identification of key stakeholders with frequent communication identified areas in need of expanded resources and addressed early ethical concerns, while local implementation efforts supported operationalization of existing infrastructure for TA-NRP procurements.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
