{"title":"Atypical PC-BPPV - Cupulolithiasis and Short-Arm Canalithiasis: A Retrospective Observational Study.","authors":"Janet O Helminski","doi":"10.1097/NPT.0000000000000494","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Atypical posterior canal (pc) benign paroxysmal positional vertigo (BPPV) may be caused by cupulolithiasis (cu), short arm canalithiasis (ca), or jam. The purpose of this study was to describe the clinical presentation and differential diagnosis of pc-BPPV-cu and short arm canalithiasis.</p><p><strong>Methods: </strong>This retrospective observation study identified persons with atypical pc-BPPV based on history and findings from four positional tests. Patterns of nystagmus suggested canal involved and mechanism of BPPV. Interventions included canalith repositioning procedures (CRP).</p><p><strong>Results: </strong>Fifteen persons, 17 episodes of care, met inclusion criteria, 65% referred following unsuccessful CRPs. Symptoms included persistent, non-positional unsteadiness, \"floating\" sensation, with half experiencing nausea/vomiting. Downbeat nystagmus with/without torsion in Dix-Hallpike (DH) and Straight Head Hang (SHH) position and no nystagmus upon sitting up, occurred in 76% of persons attributed to pc-BPPV-cu. Upbeat nystagmus with/without torsion and vertigo/retropulsion upon sitting up, occurred in 24% attributed to pc-BPPV-ca short arm. During SHH, canal conversion from pc-BPPV-cu to long arm canalithiasis occurred in 31%. The Half-Hallpike position identified pc-BPPV-cu in 71%. The Inverted Release position identified pc-BPPV-cu adjacent short arm and pc-BPPV-ca short arm.</p><p><strong>Discussion and conclusion: </strong>Persistent, peripheral nystagmus that is downbeat or downbeat/torsion away from involved ear in provoking positions and no nystagmus sitting up, may be attributed to pc-BPPV-cu, and nystagmus that is upbeat or upbeat/torsion towards involved ear upon sitting up may be attributed to pc-BPPV-ca short arm. Both are effectively treated with canal- and mechanism-specific CRPs.</p><p><strong>Video abstract available: </strong>for more insights from the authors (see the Video, Supplemental Digital Content 1 available at: (http://links.lww.com/JNPT/A487).</p>","PeriodicalId":49030,"journal":{"name":"Journal of Neurologic Physical Therapy","volume":"49 1","pages":"51-61"},"PeriodicalIF":4.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11594558/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurologic Physical Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/NPT.0000000000000494","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/16 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: Atypical posterior canal (pc) benign paroxysmal positional vertigo (BPPV) may be caused by cupulolithiasis (cu), short arm canalithiasis (ca), or jam. The purpose of this study was to describe the clinical presentation and differential diagnosis of pc-BPPV-cu and short arm canalithiasis.
Methods: This retrospective observation study identified persons with atypical pc-BPPV based on history and findings from four positional tests. Patterns of nystagmus suggested canal involved and mechanism of BPPV. Interventions included canalith repositioning procedures (CRP).
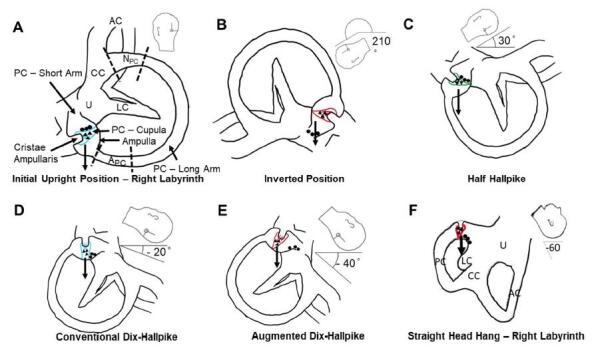
Results: Fifteen persons, 17 episodes of care, met inclusion criteria, 65% referred following unsuccessful CRPs. Symptoms included persistent, non-positional unsteadiness, "floating" sensation, with half experiencing nausea/vomiting. Downbeat nystagmus with/without torsion in Dix-Hallpike (DH) and Straight Head Hang (SHH) position and no nystagmus upon sitting up, occurred in 76% of persons attributed to pc-BPPV-cu. Upbeat nystagmus with/without torsion and vertigo/retropulsion upon sitting up, occurred in 24% attributed to pc-BPPV-ca short arm. During SHH, canal conversion from pc-BPPV-cu to long arm canalithiasis occurred in 31%. The Half-Hallpike position identified pc-BPPV-cu in 71%. The Inverted Release position identified pc-BPPV-cu adjacent short arm and pc-BPPV-ca short arm.
Discussion and conclusion: Persistent, peripheral nystagmus that is downbeat or downbeat/torsion away from involved ear in provoking positions and no nystagmus sitting up, may be attributed to pc-BPPV-cu, and nystagmus that is upbeat or upbeat/torsion towards involved ear upon sitting up may be attributed to pc-BPPV-ca short arm. Both are effectively treated with canal- and mechanism-specific CRPs.
Video abstract available: for more insights from the authors (see the Video, Supplemental Digital Content 1 available at: (http://links.lww.com/JNPT/A487).
期刊介绍:
The Journal of Neurologic Physical Therapy (JNPT) is an indexed resource for dissemination of research-based evidence related to neurologic physical therapy intervention. High standards of quality are maintained through a rigorous, double-blinded, peer-review process and adherence to standards recommended by the International Committee of Medical Journal Editors. With an international editorial board made up of preeminent researchers and clinicians, JNPT publishes articles of global relevance for examination, evaluation, prognosis, intervention, and outcomes for individuals with movement deficits due to neurologic conditions. Through systematic reviews, research articles, case studies, and clinical perspectives, JNPT promotes the integration of evidence into theory, education, research, and practice of neurologic physical therapy, spanning the continuum from pathophysiology to societal participation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
