A Machine Learning Approach for Predicting In-Hospital Cardiac Arrest Using Single-Day Vital Signs, Laboratory Test Results, and International Classification of Disease-10 Block for Diagnosis.
{"title":"A Machine Learning Approach for Predicting In-Hospital Cardiac Arrest Using Single-Day Vital Signs, Laboratory Test Results, and International Classification of Disease-10 Block for Diagnosis.","authors":"Haeil Park, Chan Seok Park","doi":"10.3343/alm.2024.0315","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Predicting in-hospital cardiac arrest (IHCA) is crucial for potentially reducing mortality and improving patient outcomes. However, most models, which rely solely on vital signs, may not comprehensively capture the patients' risk profiles. We aimed to improve IHCA predictions by combining vital sign indicators with laboratory test results and, optionally, International Classification of Disease-10 block for diagnosis (ICD10BD).</p><p><strong>Methods: </strong>We conducted a retrospective cohort study in the general ward (GW) and intensive care unit (ICU) of a 680-bed secondary healthcare institution. We included 62,061 adults admitted to the Department of Internal Medicine from January 2010 to August 2022. IHCAs were identified based on cardiopulmonary resuscitation prescriptions. Patient-days within three days preceding IHCAs were labeled as case days; all others were control days. The eXtreme Gradient Boosting (XGBoost) model was trained using daily vital signs, 14 laboratory test results, and ICD10BD.</p><p><strong>Results: </strong>In the GW, among 1,299,448 patient-days from 62,038 patients, 1,367 days linked to 713 patients were cases. In the ICU, among 117,190 patient-days from 16,881 patients, 1,119 days from 444 patients were cases. The area under the ROC curve for IHCA prediction model was 0.934 and 0.896 in the GW and ICU, respectively, using the combination of vital signs, laboratory test results, and ICD10BD; 0.925 and 0.878, respectively, with vital signs and laboratory test results; and 0.839 and 0.828, respectively, with only vital signs.</p><p><strong>Conclusions: </strong>Incorporating laboratory test results or combining laboratory test results and ICD10BD with vital signs as predictor variables in the XGBoost model potentially enhances clinical decision-making and improves patient outcomes in hospital settings.</p>","PeriodicalId":8421,"journal":{"name":"Annals of Laboratory Medicine","volume":" ","pages":"209-217"},"PeriodicalIF":3.9000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11788698/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Laboratory Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3343/alm.2024.0315","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/13 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICAL LABORATORY TECHNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Predicting in-hospital cardiac arrest (IHCA) is crucial for potentially reducing mortality and improving patient outcomes. However, most models, which rely solely on vital signs, may not comprehensively capture the patients' risk profiles. We aimed to improve IHCA predictions by combining vital sign indicators with laboratory test results and, optionally, International Classification of Disease-10 block for diagnosis (ICD10BD).
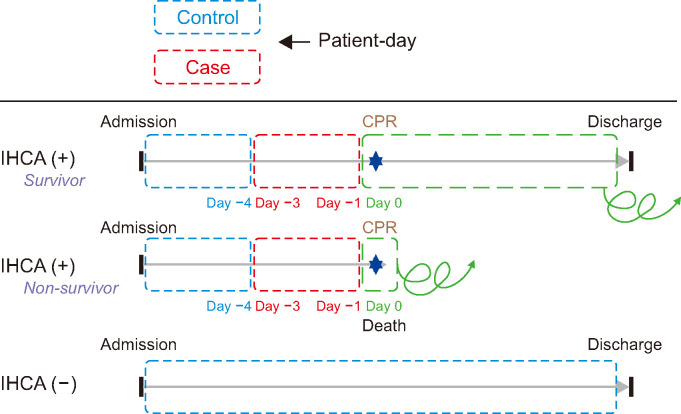
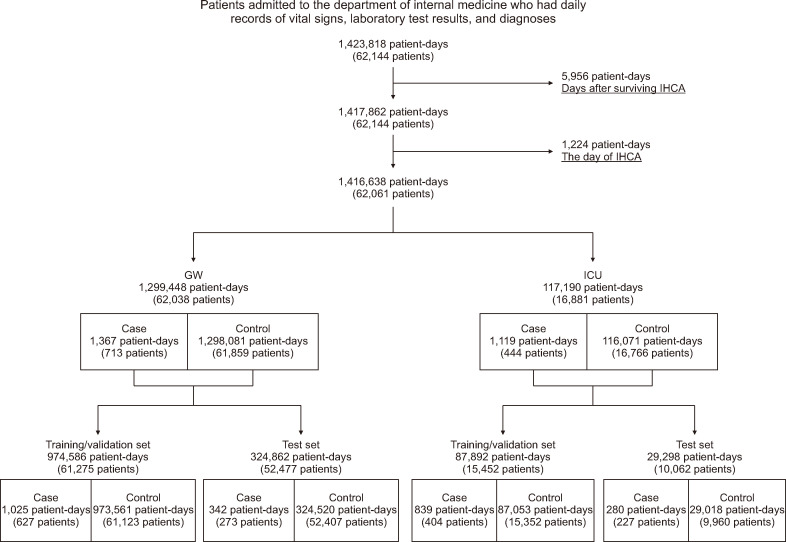
Methods: We conducted a retrospective cohort study in the general ward (GW) and intensive care unit (ICU) of a 680-bed secondary healthcare institution. We included 62,061 adults admitted to the Department of Internal Medicine from January 2010 to August 2022. IHCAs were identified based on cardiopulmonary resuscitation prescriptions. Patient-days within three days preceding IHCAs were labeled as case days; all others were control days. The eXtreme Gradient Boosting (XGBoost) model was trained using daily vital signs, 14 laboratory test results, and ICD10BD.
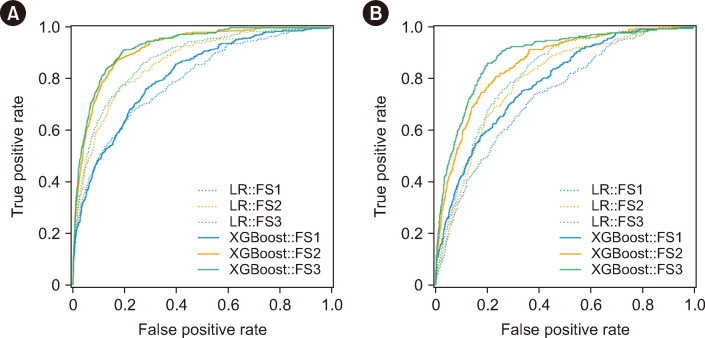
Results: In the GW, among 1,299,448 patient-days from 62,038 patients, 1,367 days linked to 713 patients were cases. In the ICU, among 117,190 patient-days from 16,881 patients, 1,119 days from 444 patients were cases. The area under the ROC curve for IHCA prediction model was 0.934 and 0.896 in the GW and ICU, respectively, using the combination of vital signs, laboratory test results, and ICD10BD; 0.925 and 0.878, respectively, with vital signs and laboratory test results; and 0.839 and 0.828, respectively, with only vital signs.
Conclusions: Incorporating laboratory test results or combining laboratory test results and ICD10BD with vital signs as predictor variables in the XGBoost model potentially enhances clinical decision-making and improves patient outcomes in hospital settings.
期刊介绍:
Annals of Laboratory Medicine is the official journal of Korean Society for Laboratory Medicine. The journal title has been recently changed from the Korean Journal of Laboratory Medicine (ISSN, 1598-6535) from the January issue of 2012. The JCR 2017 Impact factor of Ann Lab Med was 1.916.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
