Mike Wenzel, Benedikt Hoeh, Clara Humke, Maria Welte, Cristina Cano Garcia, Carolin Siech, Fred Saad, Pierre I Karakiewcz, Derya Tilki, Thomas Steuber, Markus Graefen, Miriam Traumann, Felix K H Chun, Philipp Mandel
{"title":"Administration and cancer-control outcomes of bone-modifying agents in real-world patients with metastatic castration-resistant prostate cancer.","authors":"Mike Wenzel, Benedikt Hoeh, Clara Humke, Maria Welte, Cristina Cano Garcia, Carolin Siech, Fred Saad, Pierre I Karakiewcz, Derya Tilki, Thomas Steuber, Markus Graefen, Miriam Traumann, Felix K H Chun, Philipp Mandel","doi":"10.1093/jbmrpl/ziae157","DOIUrl":null,"url":null,"abstract":"<p><p>Hormonal agents administered for metastatic castration-resistant prostate cancer (mCRPC) may lead to osteoporosis, skeletal events, reduced quality of life, and even reduced overall survival (OS). Bone-modifying agents may prevent those events but their effect on cancer-control outcomes remains uncertain. Relying on our institutional tertiary-care database, we explored the effect of bone-modifying agents (bisphosphonates such as zoledronic acid and denosumab) on OS and progression-free survival in patients with mCRPC with at least 1 bone metastasis using Kaplan-Meyer estimates and Cox regression models. Of 420 patients with mCRPC, 60% received bone-modifying agents who were younger (68 vs 69 years), with more systemic treatment lines for mCRPC (3 vs 2), and a higher proportion of initial de novo metastatic disease (72% vs 62%, all <i>p</i> ≤ .04) than patients without bone-modifying agents. In progression-free survival analyses, no significant differences were observed between both groups. In OS analyses, significant median OS differences were observed in favor of patients with bone-modifying agents (58 vs 45 months; hazard ratio [HR]: 0.66), even after multivariable adjustment (HR: 0.37; both <i>p</i> ≤ .01). In bone-modifying agent-stratified analyses, 57% received denosumab vs 43% bisphosphonates, with a significantly higher rate of Eastern Cooperative Oncology Group status of ≥2 in the bisphosphonates group. In progression-free and OS analyses, no significant differences were observed between bisphosphonates and denosumab patients, with numerically better results in progression-free survival analysis for denosumab after adjusting for covariates. The cumulative rate of osteonecrosis of the jaw at any treatment time was 12% in both groups and significantly decreased over time. Real-world data suggest a relatively low administration rate of bone-modifying agents in patients with osseous mCRPC. However, real-world data also suggest an OS benefit when bone-modifying agents are used, even after controlling for possible confounding patient and tumor characteristics.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"9 1","pages":"ziae157"},"PeriodicalIF":2.4000,"publicationDate":"2024-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11646308/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae157","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
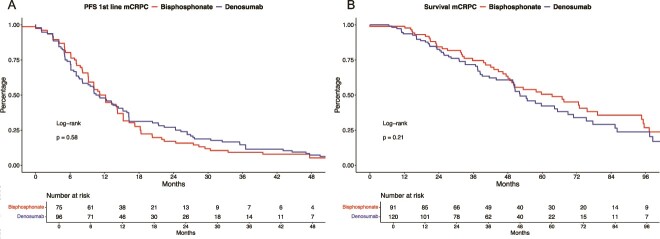
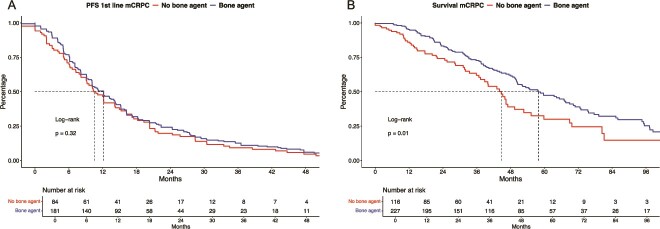
Hormonal agents administered for metastatic castration-resistant prostate cancer (mCRPC) may lead to osteoporosis, skeletal events, reduced quality of life, and even reduced overall survival (OS). Bone-modifying agents may prevent those events but their effect on cancer-control outcomes remains uncertain. Relying on our institutional tertiary-care database, we explored the effect of bone-modifying agents (bisphosphonates such as zoledronic acid and denosumab) on OS and progression-free survival in patients with mCRPC with at least 1 bone metastasis using Kaplan-Meyer estimates and Cox regression models. Of 420 patients with mCRPC, 60% received bone-modifying agents who were younger (68 vs 69 years), with more systemic treatment lines for mCRPC (3 vs 2), and a higher proportion of initial de novo metastatic disease (72% vs 62%, all p ≤ .04) than patients without bone-modifying agents. In progression-free survival analyses, no significant differences were observed between both groups. In OS analyses, significant median OS differences were observed in favor of patients with bone-modifying agents (58 vs 45 months; hazard ratio [HR]: 0.66), even after multivariable adjustment (HR: 0.37; both p ≤ .01). In bone-modifying agent-stratified analyses, 57% received denosumab vs 43% bisphosphonates, with a significantly higher rate of Eastern Cooperative Oncology Group status of ≥2 in the bisphosphonates group. In progression-free and OS analyses, no significant differences were observed between bisphosphonates and denosumab patients, with numerically better results in progression-free survival analysis for denosumab after adjusting for covariates. The cumulative rate of osteonecrosis of the jaw at any treatment time was 12% in both groups and significantly decreased over time. Real-world data suggest a relatively low administration rate of bone-modifying agents in patients with osseous mCRPC. However, real-world data also suggest an OS benefit when bone-modifying agents are used, even after controlling for possible confounding patient and tumor characteristics.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
