Nasruddin Sabrie, Nikko Gimpaya, Kareem Khalaf, Maya Deeb, Wedad Mhalawi, Michael Meleka, Daniel C Tham, Ahmed H Mokhtar, Caleb Na, Sophia P Abal, Sharan B Malipatil, Sarang Gupta, Sechiv Jugnundan, Deiya Chopra, Rishad Khan, Natalia C Calo, Christopher W Teshima, Gary R May, Jeffrey D Mosko, Samir C Grover
{"title":"Outcomes of endoscopic retrograde cholangiopancreatography performed in the AM versus PM: does procedural timing matter?","authors":"Nasruddin Sabrie, Nikko Gimpaya, Kareem Khalaf, Maya Deeb, Wedad Mhalawi, Michael Meleka, Daniel C Tham, Ahmed H Mokhtar, Caleb Na, Sophia P Abal, Sharan B Malipatil, Sarang Gupta, Sechiv Jugnundan, Deiya Chopra, Rishad Khan, Natalia C Calo, Christopher W Teshima, Gary R May, Jeffrey D Mosko, Samir C Grover","doi":"10.1093/jcag/gwae028","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>ERCP is a technically demanding procedure that carries a high cumulative adverse event (AE) rate of >10%. Identifying risk factors for adverse events is paramount. Procedure timing, as a surrogate for endoscopist fatigue, has been shown to influence key quality metrics in colonoscopy, but data on this relationship in ERCP is sparse.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of ERCP procedures performed by 5 experienced staff endoscopists, with or without advanced endoscopy fellow (AEF) involvement, from January 1, 2010 to December 1, 2020 at St Michael's Hospital, Toronto, Ontario, a regional referral center for therapeutic endoscopy. The primary outcome was the difference in rate of selective deep, duct canulation between AM and PM procedures.</p><p><strong>Results: </strong>A total of 5672 ERCP procedures were eligible for inclusion. 2793 (49.2%) procedures were performed in the AM and 2879 procedures (50.8%) were performed in the PM. We found no significant difference in the rate of selective ductal cannulation between AM and PM procedures in the unadjusted (82.8% AM vs. 83.1% <i>P</i>-value = .79) or adjusted (OR = 0.98, 95% CI, 0.85-1.12, <i>P</i>-value = .72) analyses. We found no significant difference in the mean procedural duration or rate of perforation between AM and PM procedures. The rate of immediate bleeding was slightly higher in the AM cohort.</p><p><strong>Conclusion: </strong>In our single-center retrospective study, ERCP quality, including selective cannulation rates and immediate adverse events were not significantly different in procedures performed in the morning compared to those performed in the afternoon.</p>","PeriodicalId":17263,"journal":{"name":"Journal of the Canadian Association of Gastroenterology","volume":"7 6","pages":"411-415"},"PeriodicalIF":2.7000,"publicationDate":"2024-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11637997/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Canadian Association of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jcag/gwae028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: ERCP is a technically demanding procedure that carries a high cumulative adverse event (AE) rate of >10%. Identifying risk factors for adverse events is paramount. Procedure timing, as a surrogate for endoscopist fatigue, has been shown to influence key quality metrics in colonoscopy, but data on this relationship in ERCP is sparse.
Methods: We conducted a retrospective cohort study of ERCP procedures performed by 5 experienced staff endoscopists, with or without advanced endoscopy fellow (AEF) involvement, from January 1, 2010 to December 1, 2020 at St Michael's Hospital, Toronto, Ontario, a regional referral center for therapeutic endoscopy. The primary outcome was the difference in rate of selective deep, duct canulation between AM and PM procedures.
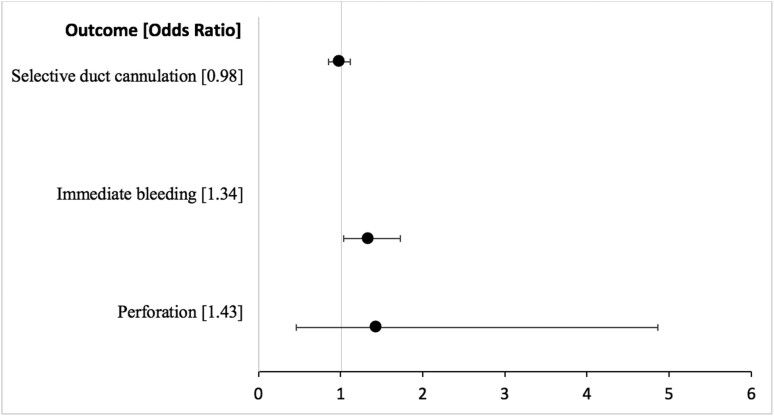
Results: A total of 5672 ERCP procedures were eligible for inclusion. 2793 (49.2%) procedures were performed in the AM and 2879 procedures (50.8%) were performed in the PM. We found no significant difference in the rate of selective ductal cannulation between AM and PM procedures in the unadjusted (82.8% AM vs. 83.1% P-value = .79) or adjusted (OR = 0.98, 95% CI, 0.85-1.12, P-value = .72) analyses. We found no significant difference in the mean procedural duration or rate of perforation between AM and PM procedures. The rate of immediate bleeding was slightly higher in the AM cohort.
Conclusion: In our single-center retrospective study, ERCP quality, including selective cannulation rates and immediate adverse events were not significantly different in procedures performed in the morning compared to those performed in the afternoon.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
