Eliza C Miller MD , Patrick Conley MS , Mohammad Alirezaei MD , Katrin Wolfova , Mitzi M Gonzales PhD , Zaldy S Tan MD , Sarah E Tom PhD , Lynn M Yee MD , Prof Adam M Brickman PhD , Natalie A Bello MD
{"title":"Associations between adverse pregnancy outcomes and cognitive impairment and dementia: a systematic review and meta-analysis","authors":"Eliza C Miller MD , Patrick Conley MS , Mohammad Alirezaei MD , Katrin Wolfova , Mitzi M Gonzales PhD , Zaldy S Tan MD , Sarah E Tom PhD , Lynn M Yee MD , Prof Adam M Brickman PhD , Natalie A Bello MD","doi":"10.1016/j.lanhl.2024.100660","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Individuals with adverse pregnancy outcomes have an increased risk of cerebrovascular disease, but the association between adverse pregnancy outcomes and cognitive impairment and dementia is less well established. We aimed to synthesise, combine, and assess the growing body of data examining the associations between adverse pregnancy outcomes and mild cognitive impairment and dementia in parous women.</div></div><div><h3>Methods</h3><div>In this systematic review and meta-analysis, we searched PubMed (MEDLINE), Web of Science, and Embase from database inception up to July 18, 2024, with no language restrictions, for observational studies or clinical trials that reported mild cognitive impairment or dementia as outcomes and included female individuals or women who had an adverse pregnancy outcome, including hypertensive disorders of pregnancy, gestational diabetes, stillbirth, fetal growth restriction, preterm birth, or placental abruption. We excluded studies of men, nulliparous women, women with pre-pregnancy conditions associated with impaired cognition, and studies examining cognitive impairment within 6 months of pregnancy. Database searches were supplemented by manual review of the reference lists of included studies. If studies met eligibility criteria but did not have sufficient data for meta-analysis (ie, did not report a summary statistic or a hazard ratio [HR] for outcome estimation), they were included in the systematic review and excluded from the meta-analysis. After removing duplicates, two investigators independently screened titles and abstracts using Covidence software, with potentially eligible studies undergoing full-text review by the same reviewers, with further review by a third reviewer and disagreements resolved by discussion and group consensus. Study quality was assessed and summary statistics extracted by two reviewers independently. The primary outcomes of our study were mild cognitive impairment, all-cause dementia, Alzheimer’s disease, and vascular dementia. Heterogeneity was measured using the Q test and <em>I</em><sup>2</sup> statistic, and we used random-effects models with inverse-variance weighting to assess the association between adverse pregnancy outcome and primary outcomes with sufficient meta-analysable data via pooled adjusted HRs and 95% CIs. The study protocol was registered with PROSPERO, CRD42023453511.</div></div><div><h3>Findings</h3><div>Of 11 251 publications identified, 15 studies (including 7 347 202 participants) met inclusion criteria for the systematic review, and 11 studies (6 263 431 participants) had sufficient data for meta-analysis. A history of any adverse pregnancy outcome was associated with higher risk of all-cause dementia (adjusted HR 1·32 [95% CI 1·17–1·49]; <em>I</em><sup>2</sup>= 80%), Alzheimer’s disease (1·26 [1·04–1·53]; <em>I</em><sup>2</sup>=63%), and vascular dementia (1·94 [1·70–2·21]; <em>I</em><sup>2</sup>=0%). A history of any hypertensive disorder of pregnancy was significantly associated with all-cause dementia (1·32 [1·11–1·57]; <em>I</em><sup>2</sup>=74%) and vascular dementia (1·78 [1·46–2·17]; <em>I</em><sup>2</sup>=0%), but not Alzheimer’s disease (1·24 [0·98–1·57]; <em>I</em><sup>2</sup>=66%). Stillbirth was not significantly associated with higher risk of all-cause dementia (1·26 [95% CI 0·93–1·71]; <em>I</em><sup>2</sup>=62%). In individual studies, similar effect directions were observed for preterm birth and fetal growth restriction, but data were insufficient for meta-analysis.</div></div><div><h3>Interpretation</h3><div>Given their increased risk of dementia, women with a history of adverse pregnancy outcomes should be evaluated for additional dementia risk factors and monitored closely for any signs of cognitive decline. Furthermore, to obtain more reliable findings, future studies should measure both exposures and outcomes prospectively and objectively.</div></div><div><h3>Funding</h3><div>National Institutes of Health, National Institute of Neurological Disorders and Stroke, National Institute on Aging, and National Heart, Lung and Blood Institute.</div></div>","PeriodicalId":34394,"journal":{"name":"Lancet Healthy Longevity","volume":"5 12","pages":"Article 100660"},"PeriodicalIF":14.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11726346/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lancet Healthy Longevity","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666756824001867","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Individuals with adverse pregnancy outcomes have an increased risk of cerebrovascular disease, but the association between adverse pregnancy outcomes and cognitive impairment and dementia is less well established. We aimed to synthesise, combine, and assess the growing body of data examining the associations between adverse pregnancy outcomes and mild cognitive impairment and dementia in parous women.
Methods
In this systematic review and meta-analysis, we searched PubMed (MEDLINE), Web of Science, and Embase from database inception up to July 18, 2024, with no language restrictions, for observational studies or clinical trials that reported mild cognitive impairment or dementia as outcomes and included female individuals or women who had an adverse pregnancy outcome, including hypertensive disorders of pregnancy, gestational diabetes, stillbirth, fetal growth restriction, preterm birth, or placental abruption. We excluded studies of men, nulliparous women, women with pre-pregnancy conditions associated with impaired cognition, and studies examining cognitive impairment within 6 months of pregnancy. Database searches were supplemented by manual review of the reference lists of included studies. If studies met eligibility criteria but did not have sufficient data for meta-analysis (ie, did not report a summary statistic or a hazard ratio [HR] for outcome estimation), they were included in the systematic review and excluded from the meta-analysis. After removing duplicates, two investigators independently screened titles and abstracts using Covidence software, with potentially eligible studies undergoing full-text review by the same reviewers, with further review by a third reviewer and disagreements resolved by discussion and group consensus. Study quality was assessed and summary statistics extracted by two reviewers independently. The primary outcomes of our study were mild cognitive impairment, all-cause dementia, Alzheimer’s disease, and vascular dementia. Heterogeneity was measured using the Q test and I2 statistic, and we used random-effects models with inverse-variance weighting to assess the association between adverse pregnancy outcome and primary outcomes with sufficient meta-analysable data via pooled adjusted HRs and 95% CIs. The study protocol was registered with PROSPERO, CRD42023453511.
Findings
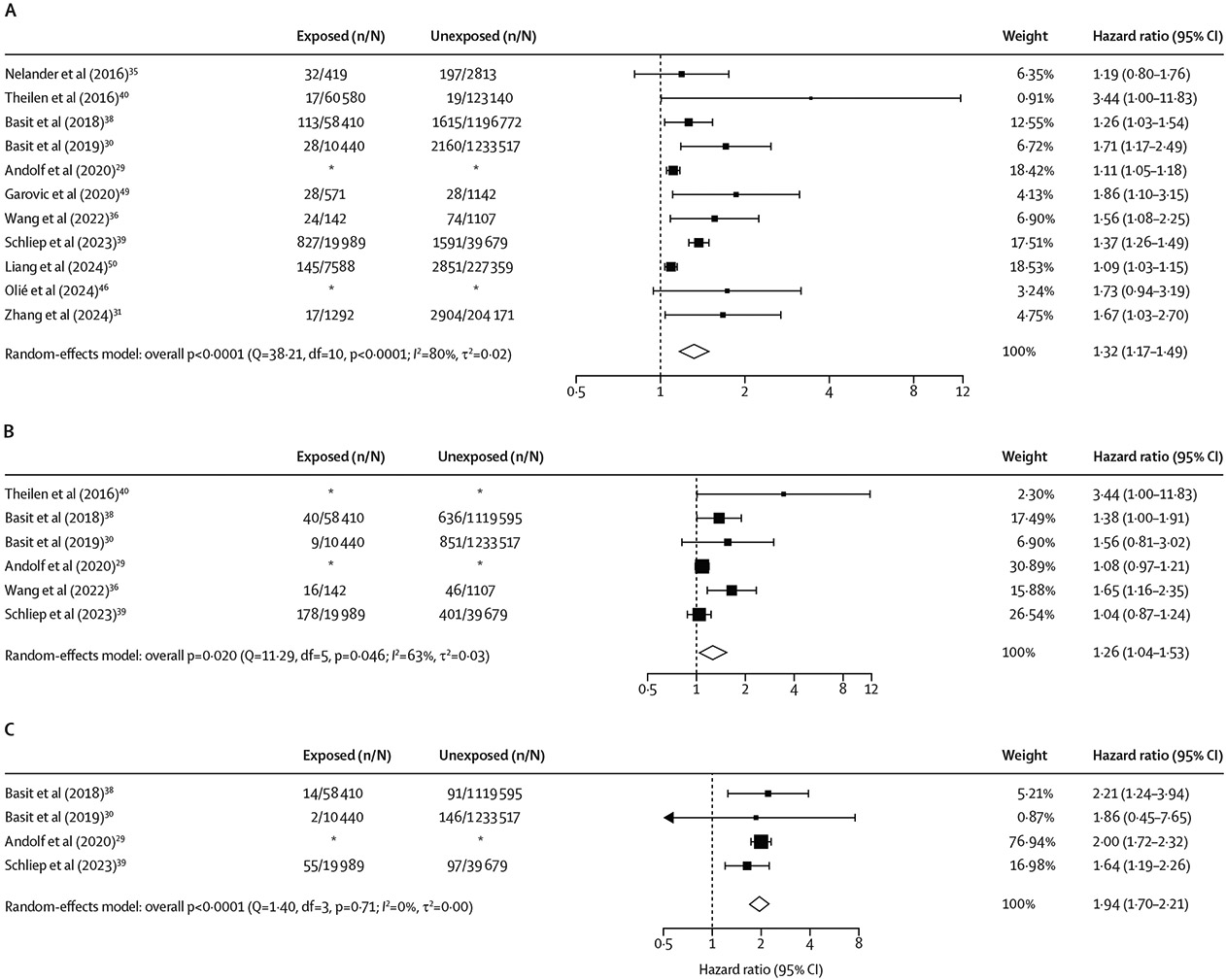
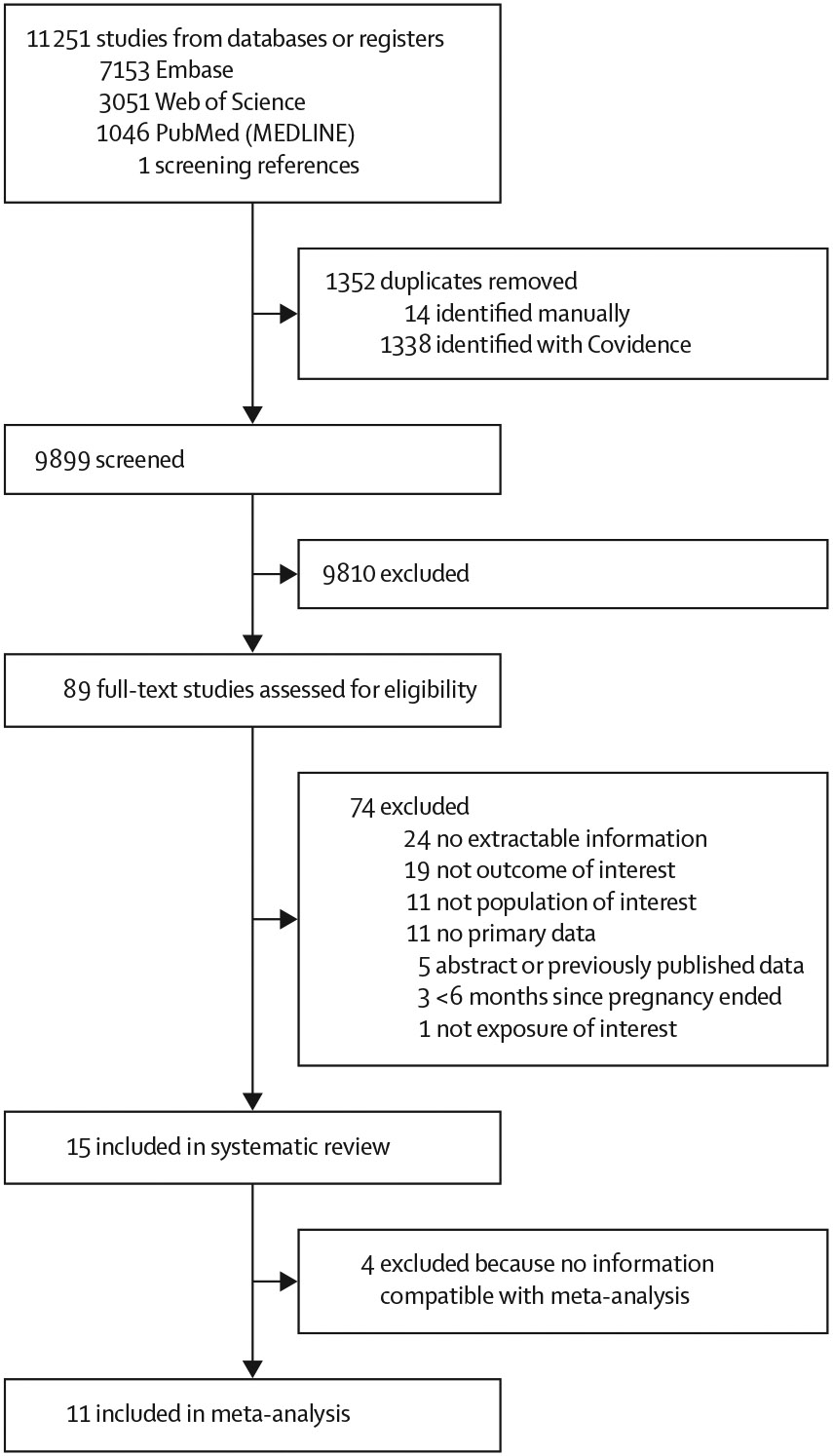
Of 11 251 publications identified, 15 studies (including 7 347 202 participants) met inclusion criteria for the systematic review, and 11 studies (6 263 431 participants) had sufficient data for meta-analysis. A history of any adverse pregnancy outcome was associated with higher risk of all-cause dementia (adjusted HR 1·32 [95% CI 1·17–1·49]; I2= 80%), Alzheimer’s disease (1·26 [1·04–1·53]; I2=63%), and vascular dementia (1·94 [1·70–2·21]; I2=0%). A history of any hypertensive disorder of pregnancy was significantly associated with all-cause dementia (1·32 [1·11–1·57]; I2=74%) and vascular dementia (1·78 [1·46–2·17]; I2=0%), but not Alzheimer’s disease (1·24 [0·98–1·57]; I2=66%). Stillbirth was not significantly associated with higher risk of all-cause dementia (1·26 [95% CI 0·93–1·71]; I2=62%). In individual studies, similar effect directions were observed for preterm birth and fetal growth restriction, but data were insufficient for meta-analysis.
Interpretation
Given their increased risk of dementia, women with a history of adverse pregnancy outcomes should be evaluated for additional dementia risk factors and monitored closely for any signs of cognitive decline. Furthermore, to obtain more reliable findings, future studies should measure both exposures and outcomes prospectively and objectively.
Funding
National Institutes of Health, National Institute of Neurological Disorders and Stroke, National Institute on Aging, and National Heart, Lung and Blood Institute.
期刊介绍:
The Lancet Healthy Longevity, a gold open-access journal, focuses on clinically-relevant longevity and healthy aging research. It covers early-stage clinical research on aging mechanisms, epidemiological studies, and societal research on changing populations. The journal includes clinical trials across disciplines, particularly in gerontology and age-specific clinical guidelines. In line with the Lancet family tradition, it advocates for the rights of all to healthy lives, emphasizing original research likely to impact clinical practice or thinking. Clinical and policy reviews also contribute to shaping the discourse in this rapidly growing discipline.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
