Efficacy and acceptability of pharmacological interventions for tardive dyskinesia in people with schizophrenia or mood disorders: a systematic review and network meta-analysis
Marco Solmi, Michele Fornaro, Stefano Caiolo, Marialaura Lussignoli, Claudio Caiazza, Michele De Prisco, Niccolo Solini, Andrea de Bartolomeis, Felice Iasevoli, Giorgio Pigato, Cinzia Del Giovane, Andrea Cipriani, Christoph U. Correll
{"title":"Efficacy and acceptability of pharmacological interventions for tardive dyskinesia in people with schizophrenia or mood disorders: a systematic review and network meta-analysis","authors":"Marco Solmi, Michele Fornaro, Stefano Caiolo, Marialaura Lussignoli, Claudio Caiazza, Michele De Prisco, Niccolo Solini, Andrea de Bartolomeis, Felice Iasevoli, Giorgio Pigato, Cinzia Del Giovane, Andrea Cipriani, Christoph U. Correll","doi":"10.1038/s41380-024-02733-z","DOIUrl":null,"url":null,"abstract":"Tardive Dyskinesia (TD) can occur in people exposed to dopamine receptor antagonists (DRAs). Its clinical management remains challenging. We conducted a systematic review/random-effects network meta-analysis (NMA) searching PubMed/MEDLINE/PsycINFO/ClinicalTrials.gov/Cochrane Central Register (22/05/2023, pre-defined protocol https://osf.io/b52ae/ ), for randomized controlled trials (RCTs) of pharmacological/brain stimulation interventions for DRA-induced TD in adults with schizophrenia or mood disorders. Primary outcomes were TD symptom change (standardized mean difference/SMD) and all-cause discontinuation (acceptability-risk ratio/RR). Sensitivity analyses were conducted. Global, local inconsistencies, risk of bias (RoB-2 tool), and confidence in evidence (CINeMA) were measured. We included 46 trials (n = 2844, age = 52.89 ± 9.94 years, males = 59.8%, schizophrenia = 84.6%, mood disorders = 15.4%), all testing pharmacological interventions versus placebo. We identified three subnetworks. In network 1, several treatments outperformed placebo on TD symptoms with large effect sizes (k = 34, n = 2269), encompassing 22 interventions versus placebo, but 18 had 1 RCTs only, and 15 had n ≤ 20. High heterogeneity (I2 = 57.1%; tau2 = 0.0797), and global inconsistency (Q = 32.64; df = 14; p = 0.0032) emerged. No significant differences emerged in acceptability. When restricting analyses to treatments with trials with n > 20 and >1 RCT, only valbenazine (k = 5, SMD = −0.69; 95% CI = −1.00, −0.37) and vitamin E (k = 7, SMD = −0.49; 95% CI = −0.87, −0.11) were superior to placebo. Deutetrabenazine outperformed placebo considering AIMS score and in low risk of bias trials only and with a moderate effect size for 24/36 mg (k = 2, SMD = −0.57/−0.60). Confidence in findings was low for deutetrabenazine and valbenazine, very low for all others. In network 2 (k = 2, n = 63), switch to molindone (k = 1, n = 9) versus switch to haloperidol worsened TD (SMD = 1.68; 95% CI = 0.61,2.76). In network 3 (k = 3, n = 194), antipsychotic wash-out+placebo (k = 1, n = 25) versus TAU+placebo (k = 1, n = 27) worsened TD (SMD = 1.30; 95% CI = 0.36,2.23). Despite large effect sizes for some treatments with very low quality/confidence, when considering higher quality evidence only valbenazine or deutetrabenazine are evidence-based first-line treatments for TD, and potentially vitamin E as second-line. Switching to molindone and antipsychotic washout should be avoided. More treatment options and higher-quality trials are needed.","PeriodicalId":19008,"journal":{"name":"Molecular Psychiatry","volume":"30 3","pages":"1207-1222"},"PeriodicalIF":10.1000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Molecular Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41380-024-02733-z","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
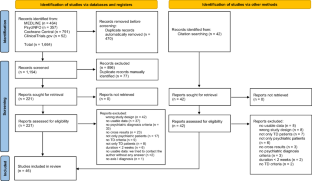
Tardive Dyskinesia (TD) can occur in people exposed to dopamine receptor antagonists (DRAs). Its clinical management remains challenging. We conducted a systematic review/random-effects network meta-analysis (NMA) searching PubMed/MEDLINE/PsycINFO/ClinicalTrials.gov/Cochrane Central Register (22/05/2023, pre-defined protocol https://osf.io/b52ae/ ), for randomized controlled trials (RCTs) of pharmacological/brain stimulation interventions for DRA-induced TD in adults with schizophrenia or mood disorders. Primary outcomes were TD symptom change (standardized mean difference/SMD) and all-cause discontinuation (acceptability-risk ratio/RR). Sensitivity analyses were conducted. Global, local inconsistencies, risk of bias (RoB-2 tool), and confidence in evidence (CINeMA) were measured. We included 46 trials (n = 2844, age = 52.89 ± 9.94 years, males = 59.8%, schizophrenia = 84.6%, mood disorders = 15.4%), all testing pharmacological interventions versus placebo. We identified three subnetworks. In network 1, several treatments outperformed placebo on TD symptoms with large effect sizes (k = 34, n = 2269), encompassing 22 interventions versus placebo, but 18 had 1 RCTs only, and 15 had n ≤ 20. High heterogeneity (I2 = 57.1%; tau2 = 0.0797), and global inconsistency (Q = 32.64; df = 14; p = 0.0032) emerged. No significant differences emerged in acceptability. When restricting analyses to treatments with trials with n > 20 and >1 RCT, only valbenazine (k = 5, SMD = −0.69; 95% CI = −1.00, −0.37) and vitamin E (k = 7, SMD = −0.49; 95% CI = −0.87, −0.11) were superior to placebo. Deutetrabenazine outperformed placebo considering AIMS score and in low risk of bias trials only and with a moderate effect size for 24/36 mg (k = 2, SMD = −0.57/−0.60). Confidence in findings was low for deutetrabenazine and valbenazine, very low for all others. In network 2 (k = 2, n = 63), switch to molindone (k = 1, n = 9) versus switch to haloperidol worsened TD (SMD = 1.68; 95% CI = 0.61,2.76). In network 3 (k = 3, n = 194), antipsychotic wash-out+placebo (k = 1, n = 25) versus TAU+placebo (k = 1, n = 27) worsened TD (SMD = 1.30; 95% CI = 0.36,2.23). Despite large effect sizes for some treatments with very low quality/confidence, when considering higher quality evidence only valbenazine or deutetrabenazine are evidence-based first-line treatments for TD, and potentially vitamin E as second-line. Switching to molindone and antipsychotic washout should be avoided. More treatment options and higher-quality trials are needed.
期刊介绍:
Molecular Psychiatry focuses on publishing research that aims to uncover the biological mechanisms behind psychiatric disorders and their treatment. The journal emphasizes studies that bridge pre-clinical and clinical research, covering cellular, molecular, integrative, clinical, imaging, and psychopharmacology levels.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
