Clinical outcomes and severity of laboratory-confirmed RSV compared with influenza, parainfluenza and human metapneumovirus in Australian children attending secondary care.
Mohinder Sarna, Huong Le, Belaynew Wasie Taye, Kathryn Glass, Avram Levy, Peter Richmond, Hannah C Moore
{"title":"Clinical outcomes and severity of laboratory-confirmed RSV compared with influenza, parainfluenza and human metapneumovirus in Australian children attending secondary care.","authors":"Mohinder Sarna, Huong Le, Belaynew Wasie Taye, Kathryn Glass, Avram Levy, Peter Richmond, Hannah C Moore","doi":"10.1136/bmjresp-2024-002613","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute lower respiratory infections (ALRIs) are a major contributor to the global infectious disease burden and a common cause of hospitalisation for children under 2 years. We compared clinical severity in children hospitalised with respiratory syncytial virus (RSV), parainfluenza virus (PIV), human metapneumovirus (hMPV) and influenza virus (IFV).</p><p><strong>Methods: </strong>We used a probabilistically linked population cohort born in Western Australia between 2010 and 2020 and hospitalised before the age of 2 years. Outcomes compared included length of hospital stay (LOS), admission to intensive care unit (ICU), need for respiratory support (RS), complex hospital course (RS, death, ICU admission or LOS >75th percentile), 7-day and 30-day mortality, hospital-in-the-home care, 30-day all-cause and ALRI-specific readmissions and emergency department presentations 14 days prior to hospitalisation. Logistic regression was used for binary outcomes, and negative binomial regression was used for discrete count variables. Incidence rates, time to RS and time to readmissions were calculated using survival analysis techniques.</p><p><strong>Results: </strong>The final cohort included 210 997 hospitalised children under 24 months of age for a total of 315 769 admissions. Infants hospitalised before 6 months had the highest rates for all virus-specific hospitalisations, particularly RSV hospitalisations (50.4 per 1000 child-years (95% CI 48.7 to 52.1)). Infants <6 months had higher odds of an ICU admission (adjusted OR (aOR) 2.39, 95% CI 1.36 to 4.19) and RS (aOR 4.68, 95% CI 2.95 to 7.44) and a complex hospital course (aOR 2.69, 95% CI 2.13 to 3.42) with RSV and four times higher hazards of requiring RS earlier (adjusted HR (aHR) 4.06, 95% CI 2.59 to 6.36). An ALRI-coded 30-day readmission was recorded in 10%-24% of virus-specific hospitalisations.</p><p><strong>Discussion: </strong>Young infants have a more severe and complex hospital course with RSV hospitalisation compared with hospitalisation with other respiratory viruses and should be prioritised for prevention measures such as the single-dose monoclonal antibody, nirsevimab.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"11 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11667329/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002613","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Acute lower respiratory infections (ALRIs) are a major contributor to the global infectious disease burden and a common cause of hospitalisation for children under 2 years. We compared clinical severity in children hospitalised with respiratory syncytial virus (RSV), parainfluenza virus (PIV), human metapneumovirus (hMPV) and influenza virus (IFV).
Methods: We used a probabilistically linked population cohort born in Western Australia between 2010 and 2020 and hospitalised before the age of 2 years. Outcomes compared included length of hospital stay (LOS), admission to intensive care unit (ICU), need for respiratory support (RS), complex hospital course (RS, death, ICU admission or LOS >75th percentile), 7-day and 30-day mortality, hospital-in-the-home care, 30-day all-cause and ALRI-specific readmissions and emergency department presentations 14 days prior to hospitalisation. Logistic regression was used for binary outcomes, and negative binomial regression was used for discrete count variables. Incidence rates, time to RS and time to readmissions were calculated using survival analysis techniques.
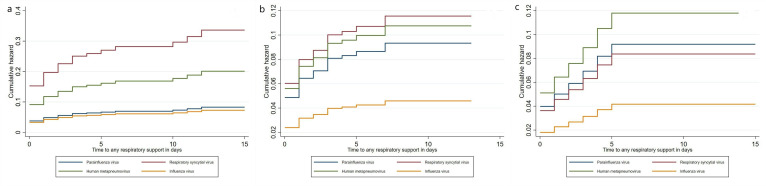
Results: The final cohort included 210 997 hospitalised children under 24 months of age for a total of 315 769 admissions. Infants hospitalised before 6 months had the highest rates for all virus-specific hospitalisations, particularly RSV hospitalisations (50.4 per 1000 child-years (95% CI 48.7 to 52.1)). Infants <6 months had higher odds of an ICU admission (adjusted OR (aOR) 2.39, 95% CI 1.36 to 4.19) and RS (aOR 4.68, 95% CI 2.95 to 7.44) and a complex hospital course (aOR 2.69, 95% CI 2.13 to 3.42) with RSV and four times higher hazards of requiring RS earlier (adjusted HR (aHR) 4.06, 95% CI 2.59 to 6.36). An ALRI-coded 30-day readmission was recorded in 10%-24% of virus-specific hospitalisations.
Discussion: Young infants have a more severe and complex hospital course with RSV hospitalisation compared with hospitalisation with other respiratory viruses and should be prioritised for prevention measures such as the single-dose monoclonal antibody, nirsevimab.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
