Roshni Vamja, Yogesh M, Monika Patel, Vijay Vala, Arya Ramachandran, Bhumika Surati, Jay Nagda
{"title":"Impact of maternal thyroid dysfunction on fetal and maternal outcomes in pregnancy: a prospective cohort study.","authors":"Roshni Vamja, Yogesh M, Monika Patel, Vijay Vala, Arya Ramachandran, Bhumika Surati, Jay Nagda","doi":"10.1186/s40842-024-00212-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Thyroid dysfunction in pregnancy can adversely impact maternal and fetal outcomes. However, the association between thyroid status and specific adverse outcomes needs clarity, especially in understudied regions.</p><p><strong>Objective: </strong>This prospective cohort study aimed to illuminate the multifaceted associations between maternal thyroid dysfunction and feto-maternal outcomes in Gujarat, India.</p><p><strong>Methods: </strong>This hospital-based cohort study recruited and monitored 500 euthyroid, 250 hypothyroid, and 150 hyperthyroid pregnant women until delivery. Maternal thyroid status was determined by serum thyroid stimulating hormone (TSH) and free thyroxine (fT4) levels. Adverse fetal outcomes included preterm birth, neonatal intensive care unit (NICU) admission, respiratory issues, and low APGAR scores. Maternal outcomes included preeclampsia, haemorrhage, hypertension, postpartum thyroiditis, and thromboembolism. Relative risks quantified associations between thyroid dysfunction and outcomes.</p><p><strong>Results: </strong>Compared to euthyroid women, hypothyroid women had a higher RR for preterm birth (RR 1.8, 95% CI 1.1-3.0), low APGAR score (RR 2.5, 95% CI 1.5-4.1), preeclampsia (RR 3.0, 95% CI 1.9-4.8), postpartum haemorrhage (RR 1.6, 95% CI 1.2-2.1), and venous thromboembolism (RR 3.1, 95% CI 1.7-5.7). Hyperthyroid women had over twice the risk of low APGAR score (RR 1.8, 95% CI 0.9-3.5), neonatal hypoglycemia (RR 1.5, 95% CI 0.5-4.3), respiratory distress (RR 1.4, 95% CI 0.7-2.8), and postpartum thyroiditis (RR 2.3, 95% CI 1.1-4.8).</p><p><strong>Conclusion: </strong>Maternal thyroid dysfunction escalates risks for adverse fetal and maternal outcomes. Thyroid monitoring and management during pregnancy are critical to mitigate complications.</p>","PeriodicalId":56339,"journal":{"name":"Clinical Diabetes and Endocrinology","volume":"10 1","pages":"50"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11658447/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Diabetes and Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40842-024-00212-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Thyroid dysfunction in pregnancy can adversely impact maternal and fetal outcomes. However, the association between thyroid status and specific adverse outcomes needs clarity, especially in understudied regions.
Objective: This prospective cohort study aimed to illuminate the multifaceted associations between maternal thyroid dysfunction and feto-maternal outcomes in Gujarat, India.
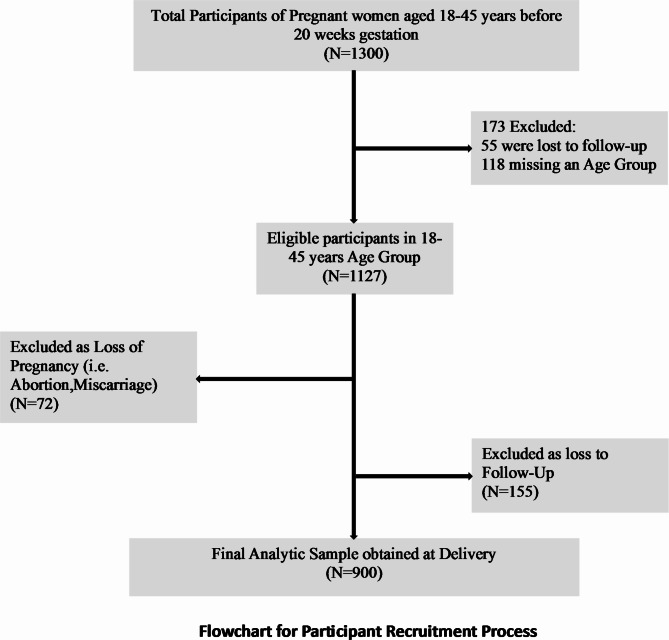
Methods: This hospital-based cohort study recruited and monitored 500 euthyroid, 250 hypothyroid, and 150 hyperthyroid pregnant women until delivery. Maternal thyroid status was determined by serum thyroid stimulating hormone (TSH) and free thyroxine (fT4) levels. Adverse fetal outcomes included preterm birth, neonatal intensive care unit (NICU) admission, respiratory issues, and low APGAR scores. Maternal outcomes included preeclampsia, haemorrhage, hypertension, postpartum thyroiditis, and thromboembolism. Relative risks quantified associations between thyroid dysfunction and outcomes.
Results: Compared to euthyroid women, hypothyroid women had a higher RR for preterm birth (RR 1.8, 95% CI 1.1-3.0), low APGAR score (RR 2.5, 95% CI 1.5-4.1), preeclampsia (RR 3.0, 95% CI 1.9-4.8), postpartum haemorrhage (RR 1.6, 95% CI 1.2-2.1), and venous thromboembolism (RR 3.1, 95% CI 1.7-5.7). Hyperthyroid women had over twice the risk of low APGAR score (RR 1.8, 95% CI 0.9-3.5), neonatal hypoglycemia (RR 1.5, 95% CI 0.5-4.3), respiratory distress (RR 1.4, 95% CI 0.7-2.8), and postpartum thyroiditis (RR 2.3, 95% CI 1.1-4.8).
Conclusion: Maternal thyroid dysfunction escalates risks for adverse fetal and maternal outcomes. Thyroid monitoring and management during pregnancy are critical to mitigate complications.
背景:妊娠期甲状腺功能障碍会对母体和胎儿的结局产生不利影响。然而,甲状腺状态和特定不良后果之间的关系需要明确,特别是在研究不足的地区。目的:本前瞻性队列研究旨在阐明在印度古吉拉特邦母亲甲状腺功能障碍和胎母结局之间的多方面联系。方法:这项以医院为基础的队列研究招募并监测了500名甲状腺功能正常、250名甲状腺功能减退和150名甲状腺功能亢进的孕妇,直至分娩。通过血清促甲状腺激素(TSH)和游离甲状腺素(fT4)水平测定母体甲状腺状态。不良胎儿结局包括早产、新生儿重症监护病房(NICU)入院、呼吸问题和低APGAR评分。产妇结局包括先兆子痫、出血、高血压、产后甲状腺炎和血栓栓塞。相对危险度量化了甲状腺功能障碍与预后之间的关系。结果:与甲状腺功能正常的女性相比,甲状腺功能低下的女性在早产(RR 1.8, 95% CI 1.1-3.0)、低APGAR评分(RR 2.5, 95% CI 1.5-4.1)、先兆子痫(RR 3.0, 95% CI 1.9-4.8)、产后出血(RR 1.6, 95% CI 1.2-2.1)和静脉血栓栓塞(RR 3.1, 95% CI 1.7-5.7)方面具有更高的RR。甲状腺功能亢进妇女APGAR评分低(RR 1.8, 95% CI 0.9-3.5)、新生儿低血糖(RR 1.5, 95% CI 0.5-4.3)、呼吸窘迫(RR 1.4, 95% CI 0.7-2.8)和产后甲状腺炎(RR 2.3, 95% CI 1.1-4.8)的风险超过两倍。结论:母体甲状腺功能障碍增加了胎儿和母体不良结局的风险。妊娠期甲状腺监测和管理对减轻并发症至关重要。
期刊介绍:
Clinical Diabetes and Endocrinology is an open access journal publishing within the field of diabetes and endocrine disease. The journal aims to provide a widely available resource for people working within the field of diabetes and endocrinology, in order to improve the care of people affected by these conditions. The audience includes, but is not limited to, physicians, researchers, nurses, nutritionists, pharmacists, podiatrists, psychologists, epidemiologists, exercise physiologists and health care researchers. Research articles include patient-based research (clinical trials, clinical studies, and others), translational research (translation of basic science to clinical practice, translation of clinical practice to policy and others), as well as epidemiology and health care research. Clinical articles include case reports, case seminars, consensus statements, clinical practice guidelines and evidence-based medicine. Only articles considered to contribute new knowledge to the field will be considered for publication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
