{"title":"Sepsis survivors readmitted within 30 days: outcomes of a single-center retrospective study.","authors":"Abdelrahman Nanah, Fatima Abdeljaleel, Marcos Vinícius Fernandes Garcia, Kelly Pannikodu, Mohannad Seif, Amy Flowers-Surovi, Naveen Gopal, Divyajot Sadana","doi":"10.62675/2965-2774.20240116-en","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate a cohort of sepsis survivors readmitted within 30 days postdischarge, explore the one-year mortality rate based on different causes of readmission and identify factors associated with increased one-year mortality risk among all sepsis survivors readmitted within this timeframe.</p><p><strong>Methods: </strong>This was a single-center retrospective cohort study involving adult sepsis survivors who were readmitted within 30 days of discharge. Patients were categorized into 3 groups based on the cause of readmission: same-source infectious readmission, different-source infectious readmission, and noninfectious readmission. The outcome of interest was all-cause one-year mortality. Cox proportional hazard analysis was performed to compare factors associated with one-year mortality.</p><p><strong>Results: </strong>Of the 1,666 patients admitted with sepsis, 243 (14.5%) were readmitted within 30 days. Readmissions were due to same-source infections (40.7%), different-source infections (21.4%), or noninfectious causes (37.9%). All-cause one-year mortality was 46.9%, with no difference between the groups. Age (HR 1.02; 95%CI: 1.003 - 1.04; p = 0.01), Sequential Organ Failure Assessment score (HR 1.1; 95%CI: 1.02 - 1.18; p = 0.01), discharge to a care facility during index admission (HR 1.6; 95%CI: 1.04 - 2.40; p = 0.03), and malignancy (HR 2.3; 95%CI: 1.5 - 3.7; p < 0.001) were associated with one-year mortality.</p><p><strong>Conclusion: </strong>Thirty-day readmission in sepsis survivors was common and was associated with a 46.9% one-year mortality rate regardless of readmission cause. Quality improvement patient safety initiatives based on local institutional factors may allow for targeted interventions to improve sepsis survivor outcomes.</p>","PeriodicalId":72721,"journal":{"name":"Critical care science","volume":"36 ","pages":"e20240116en"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11812674/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.62675/2965-2774.20240116-en","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To investigate a cohort of sepsis survivors readmitted within 30 days postdischarge, explore the one-year mortality rate based on different causes of readmission and identify factors associated with increased one-year mortality risk among all sepsis survivors readmitted within this timeframe.
Methods: This was a single-center retrospective cohort study involving adult sepsis survivors who were readmitted within 30 days of discharge. Patients were categorized into 3 groups based on the cause of readmission: same-source infectious readmission, different-source infectious readmission, and noninfectious readmission. The outcome of interest was all-cause one-year mortality. Cox proportional hazard analysis was performed to compare factors associated with one-year mortality.
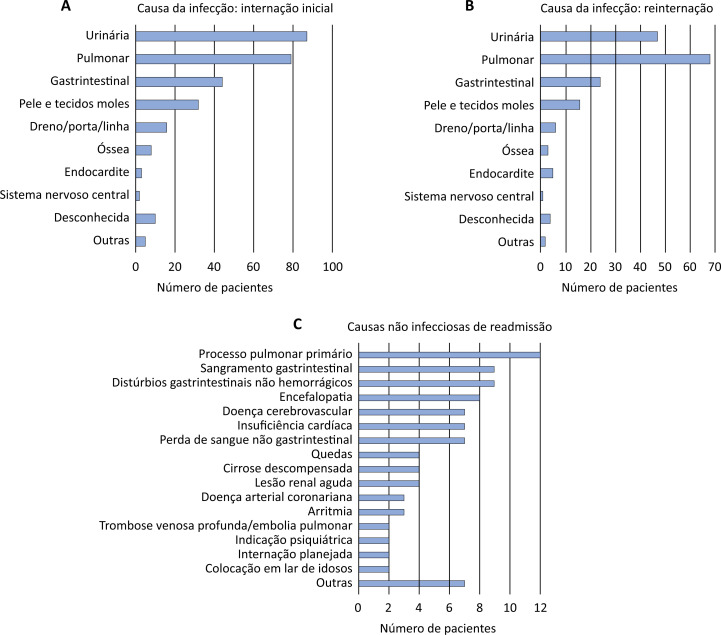
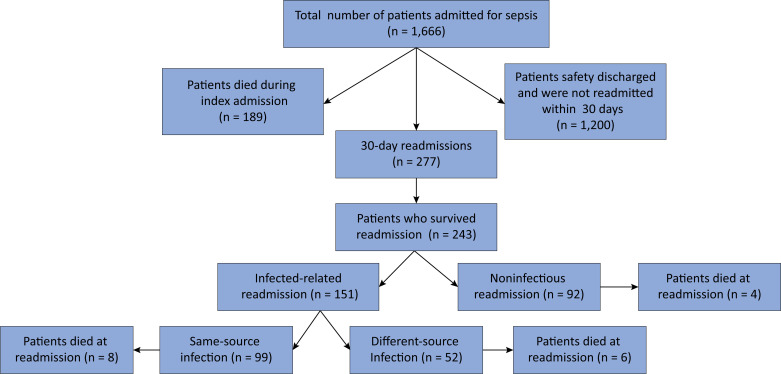
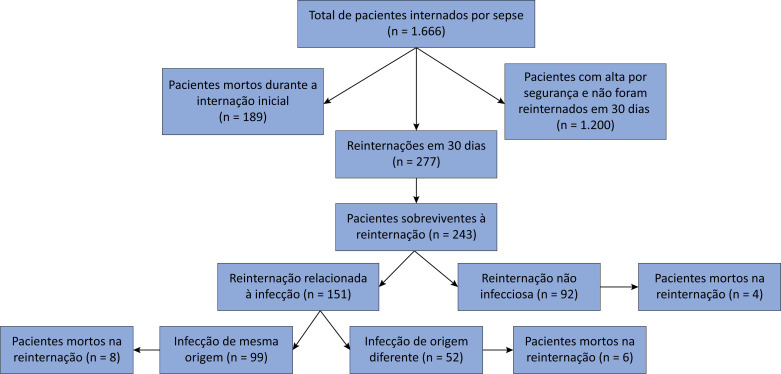
Results: Of the 1,666 patients admitted with sepsis, 243 (14.5%) were readmitted within 30 days. Readmissions were due to same-source infections (40.7%), different-source infections (21.4%), or noninfectious causes (37.9%). All-cause one-year mortality was 46.9%, with no difference between the groups. Age (HR 1.02; 95%CI: 1.003 - 1.04; p = 0.01), Sequential Organ Failure Assessment score (HR 1.1; 95%CI: 1.02 - 1.18; p = 0.01), discharge to a care facility during index admission (HR 1.6; 95%CI: 1.04 - 2.40; p = 0.03), and malignancy (HR 2.3; 95%CI: 1.5 - 3.7; p < 0.001) were associated with one-year mortality.
Conclusion: Thirty-day readmission in sepsis survivors was common and was associated with a 46.9% one-year mortality rate regardless of readmission cause. Quality improvement patient safety initiatives based on local institutional factors may allow for targeted interventions to improve sepsis survivor outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
