{"title":"Cytokine Release Syndrome After CAR T-Cell Therapy in a 35-Year-Old Patient With <i>Pneumocystis jiroveci</i> Pneumonia and Cytomegalovirus Viremia.","authors":"Kristina A Helms","doi":"10.1155/carm/6751047","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The risk of cytokine release syndrome (CRS) in patients with infections prior to chimeric antigen receptor T-cell (CAR T-cell) therapy represents an important and underreported event. Patients with active infections needing prompt CAR T-cell therapy to treat aggressive hematologic malignancies remain a clinical challenge. <b>Case Report:</b> This case describes the clinical course of a 35-year-old male patient with relapsed/refractory T-cell/histiocyte-rich large B-cell lymphoma who received axicabtagene ciloleucel. The patient developed ASTCT Grade II CRS on day +5, necessitating hospital admission and intravenous antibiotics, dexamethasone and tocilizumab. The patient was found to have a <i>Pneumocystis jirovecii</i> pneumonia (PJP) infection 3 days prior to CAR T-cell infusion and cytomegalovirus (CMV) viremia 3 days after CAR T-cell infusion. He received TMP-SMX for 21 days to treat PJP and valganciclovir to treat CMV viremia. PET/CT on day +26 demonstrated near resolution of pulmonary nodules and significant partial response of disease according to Deauville criteria. <b>Conclusion:</b> This case highlights the risk of CRS in immunocompromised patients with infections, and presents a unique case of CRS associated with PJP and CMV infections. Although the patient's clinical course was fraught with complications, he achieved a significant partial response to CAR T-cell therapy with the help of a multidisciplinary medical team.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":"2024 ","pages":"6751047"},"PeriodicalIF":0.7000,"publicationDate":"2024-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666310/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/carm/6751047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
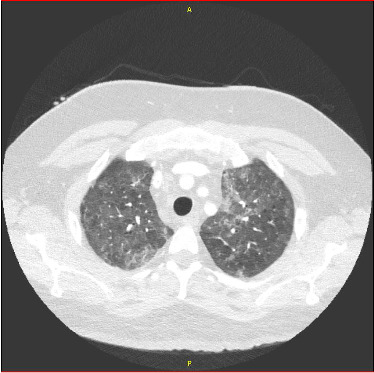
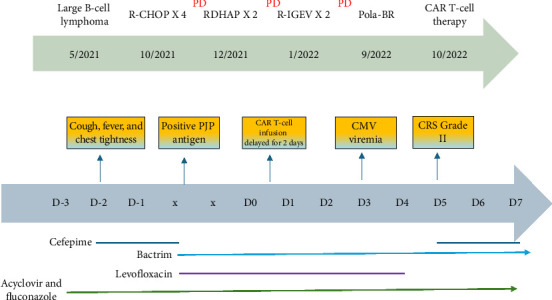
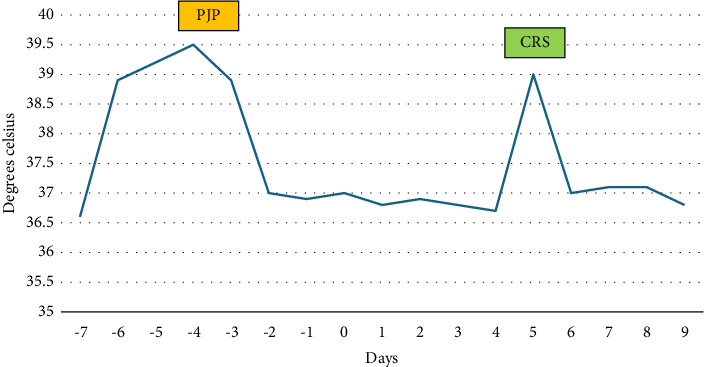
Background: The risk of cytokine release syndrome (CRS) in patients with infections prior to chimeric antigen receptor T-cell (CAR T-cell) therapy represents an important and underreported event. Patients with active infections needing prompt CAR T-cell therapy to treat aggressive hematologic malignancies remain a clinical challenge. Case Report: This case describes the clinical course of a 35-year-old male patient with relapsed/refractory T-cell/histiocyte-rich large B-cell lymphoma who received axicabtagene ciloleucel. The patient developed ASTCT Grade II CRS on day +5, necessitating hospital admission and intravenous antibiotics, dexamethasone and tocilizumab. The patient was found to have a Pneumocystis jirovecii pneumonia (PJP) infection 3 days prior to CAR T-cell infusion and cytomegalovirus (CMV) viremia 3 days after CAR T-cell infusion. He received TMP-SMX for 21 days to treat PJP and valganciclovir to treat CMV viremia. PET/CT on day +26 demonstrated near resolution of pulmonary nodules and significant partial response of disease according to Deauville criteria. Conclusion: This case highlights the risk of CRS in immunocompromised patients with infections, and presents a unique case of CRS associated with PJP and CMV infections. Although the patient's clinical course was fraught with complications, he achieved a significant partial response to CAR T-cell therapy with the help of a multidisciplinary medical team.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
