Thillagavathie Pillay, Sarah E Seaton, Miaoqing Yang, Vasiliki Bountziouka, Victor Banda, Helen Campbell, Kelvin Dawson, Bradley N Manktelow, Elizabeth S Draper, Neena Modi, Elaine M Boyle, Oliver Rivero-Arias
{"title":"Improving outcomes for very preterm babies in England: does place of birth matter? Findings from OPTI-PREM, a national cohort study.","authors":"Thillagavathie Pillay, Sarah E Seaton, Miaoqing Yang, Vasiliki Bountziouka, Victor Banda, Helen Campbell, Kelvin Dawson, Bradley N Manktelow, Elizabeth S Draper, Neena Modi, Elaine M Boyle, Oliver Rivero-Arias","doi":"10.1136/archdischild-2024-327474","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Babies born between 27<sup>+0</sup> and 31<sup>+6</sup> weeks of gestation contribute substantially towards infant mortality and morbidity. In England, their care is delivered in maternity services colocated with highly specialised neonatal intensive care units (NICU) or less specialised local neonatal units (LNU). We investigated whether birth setting offered survival and/or morbidity advantages to inform National Health Service delivery.</p><p><strong>Design: </strong>Retrospective national cohort study.</p><p><strong>Setting: </strong>LNU, NICU, England.</p><p><strong>Patients: </strong>UK National Neonatal Research Database whole population data for births between 27<sup>+0</sup> and 31<sup>+6</sup> weeks of gestation, discharged from/died within neonatal units between 1 January 2014 and 31 December 2018. We linked baby-level data to mortality information from the Office for National Statistics.</p><p><strong>Outcome measures: </strong>Death during neonatal care, up to 1 year (infant mortality), surgically treated necrotising enterocolitis, retinopathy of prematurity, severe brain injury (SBI), bronchopulmonary dysplasia.</p><p><strong>Intervention: </strong>Birth in NICU versus LNU setting. We used an instrumental variable (maternal excess travel time between the nearest NICU and LNU) estimation approach to determine treatment effect.</p><p><strong>Results: </strong>Of 18 847 babies (NICU: 10 379; LNU: 8468), 574 died in NICU/LNU care, and 121 postdischarge (infant mortality 3.7%). We found no effect of birth setting on neonatal or infant mortality. Significantly more babies born into LNU settings experienced SBI (mean difference -1.1% (99% CI -2.2% to -0.1%)). This was attenuated after excluding births at 27 weeks, and early postnatal transfers.</p><p><strong>Conclusions: </strong>In England, LNU teams should use clinical judgement, risk assessing benefits of transfer versus risk of SBI for preterm births at 27 weeks of gestation. 28 weeks of gestation is a safe threshold for preterm birth in either NICU/LNU settings.</p><p><strong>Trial registration number: </strong>NCT02994849/ISRCTN74230187.</p>","PeriodicalId":8177,"journal":{"name":"Archives of Disease in Childhood - Fetal and Neonatal Edition","volume":" ","pages":"444-451"},"PeriodicalIF":3.6000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12418565/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Disease in Childhood - Fetal and Neonatal Edition","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/archdischild-2024-327474","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Babies born between 27+0 and 31+6 weeks of gestation contribute substantially towards infant mortality and morbidity. In England, their care is delivered in maternity services colocated with highly specialised neonatal intensive care units (NICU) or less specialised local neonatal units (LNU). We investigated whether birth setting offered survival and/or morbidity advantages to inform National Health Service delivery.
Design: Retrospective national cohort study.
Setting: LNU, NICU, England.
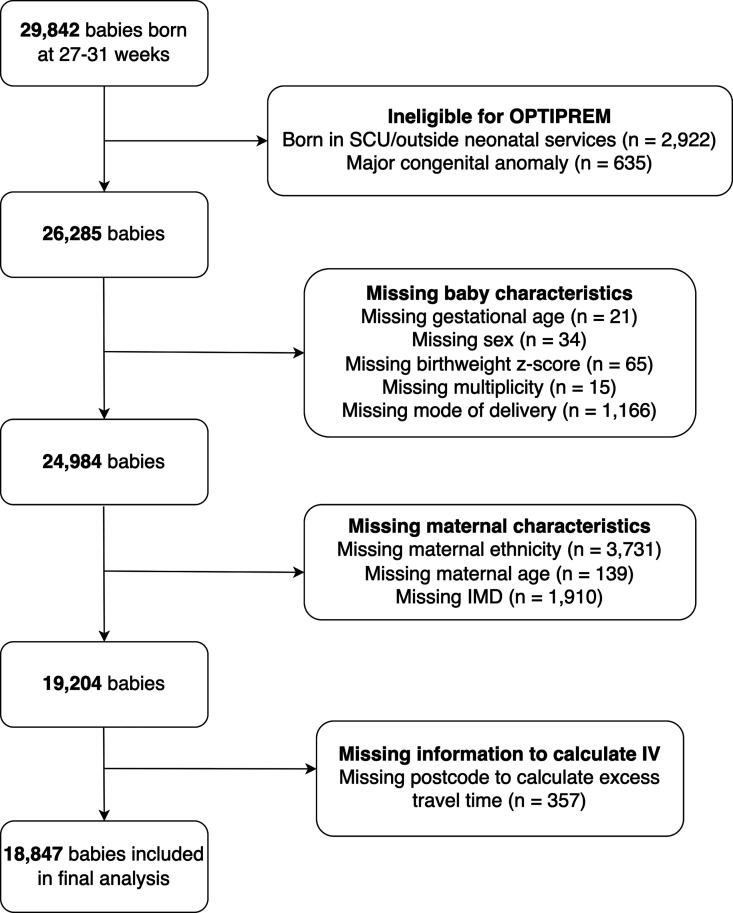
Patients: UK National Neonatal Research Database whole population data for births between 27+0 and 31+6 weeks of gestation, discharged from/died within neonatal units between 1 January 2014 and 31 December 2018. We linked baby-level data to mortality information from the Office for National Statistics.
Outcome measures: Death during neonatal care, up to 1 year (infant mortality), surgically treated necrotising enterocolitis, retinopathy of prematurity, severe brain injury (SBI), bronchopulmonary dysplasia.
Intervention: Birth in NICU versus LNU setting. We used an instrumental variable (maternal excess travel time between the nearest NICU and LNU) estimation approach to determine treatment effect.
Results: Of 18 847 babies (NICU: 10 379; LNU: 8468), 574 died in NICU/LNU care, and 121 postdischarge (infant mortality 3.7%). We found no effect of birth setting on neonatal or infant mortality. Significantly more babies born into LNU settings experienced SBI (mean difference -1.1% (99% CI -2.2% to -0.1%)). This was attenuated after excluding births at 27 weeks, and early postnatal transfers.
Conclusions: In England, LNU teams should use clinical judgement, risk assessing benefits of transfer versus risk of SBI for preterm births at 27 weeks of gestation. 28 weeks of gestation is a safe threshold for preterm birth in either NICU/LNU settings.
期刊介绍:
Archives of Disease in Childhood is an international peer review journal that aims to keep paediatricians and others up to date with advances in the diagnosis and treatment of childhood diseases as well as advocacy issues such as child protection. It focuses on all aspects of child health and disease from the perinatal period (in the Fetal and Neonatal edition) through to adolescence. ADC includes original research reports, commentaries, reviews of clinical and policy issues, and evidence reports. Areas covered include: community child health, public health, epidemiology, acute paediatrics, advocacy, and ethics.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
