Duha Zaffar MD , Aditi Rawat MD , Robert T. Chow MD , Kashif M. Munir MD
{"title":"Diabetic Ketoacidosis Without Diabetes Mellitus in Acute Pancreatitis","authors":"Duha Zaffar MD , Aditi Rawat MD , Robert T. Chow MD , Kashif M. Munir MD","doi":"10.1016/j.aace.2024.07.007","DOIUrl":null,"url":null,"abstract":"<div><h3>Background/Objective</h3><div>Diabetic ketoacidosis (DKA) is typically but not exclusively seen in patients with a history of diabetes mellitus.</div></div><div><h3>Case Report</h3><div>This is a case of 39 year-old male who was diagnosed with acute pancreatitis based on characteristic symptoms and positive CT findings on presentation. Laboratory testing revealed elevated serum glucose 251 mg/dL, low serum bicarbonate 8 mmol/L, increased anion gap 21, and elevated serum beta-hydroxybutyrate 9.62 mmol/L. Diagnosis of DKA was made, however patient did not carry a diagnosis of diabetes mellitus. His hemoglobin A1c in hospital was normal at 5.4%. Additionally, follow-up hemoglobin A1c at 4 months and 10 months postdischarge did not imply diabetes mellitus, 5.8% at both time points. The patient who was initially managed with intravenous insulin required no insulin or oral diabetic medication on discharge. All these findings argued against new onset diabetes mellitus.</div></div><div><h3>Discussion</h3><div>This case explores the potential pathophysiology that underlies this phenomenon including possible transient insulin insufficiency due to beta cell dysfunction from pancreatic inflammation. It also highlights the reversibility and transiency of possible beta cell dysfunction during acute pancreatitis and emphasizes the importance of closely assessing the patients' insulin requirements upon discharge, especially when a prior history of diabetes mellitus is absent.</div></div><div><h3>Conclusion</h3><div>DKA can occur as a rare complication of acute pancreatitis in a nondiabetic patient. Hyperglycemia associated with acute pancreatitis-induced DKA can be temporary and these patients might not necessarily require insulin upon discharge. Therefore, careful discharge planning is very important in such patients.</div></div>","PeriodicalId":7051,"journal":{"name":"AACE Clinical Case Reports","volume":"10 6","pages":"Pages 220-223"},"PeriodicalIF":1.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11680747/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AACE Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2376060524000762","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background/Objective
Diabetic ketoacidosis (DKA) is typically but not exclusively seen in patients with a history of diabetes mellitus.
Case Report
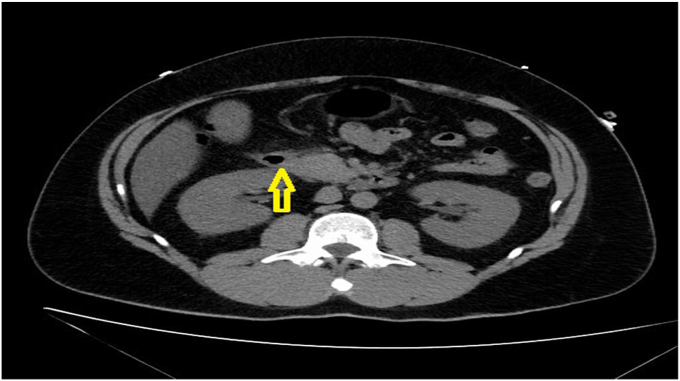
This is a case of 39 year-old male who was diagnosed with acute pancreatitis based on characteristic symptoms and positive CT findings on presentation. Laboratory testing revealed elevated serum glucose 251 mg/dL, low serum bicarbonate 8 mmol/L, increased anion gap 21, and elevated serum beta-hydroxybutyrate 9.62 mmol/L. Diagnosis of DKA was made, however patient did not carry a diagnosis of diabetes mellitus. His hemoglobin A1c in hospital was normal at 5.4%. Additionally, follow-up hemoglobin A1c at 4 months and 10 months postdischarge did not imply diabetes mellitus, 5.8% at both time points. The patient who was initially managed with intravenous insulin required no insulin or oral diabetic medication on discharge. All these findings argued against new onset diabetes mellitus.
Discussion
This case explores the potential pathophysiology that underlies this phenomenon including possible transient insulin insufficiency due to beta cell dysfunction from pancreatic inflammation. It also highlights the reversibility and transiency of possible beta cell dysfunction during acute pancreatitis and emphasizes the importance of closely assessing the patients' insulin requirements upon discharge, especially when a prior history of diabetes mellitus is absent.
Conclusion
DKA can occur as a rare complication of acute pancreatitis in a nondiabetic patient. Hyperglycemia associated with acute pancreatitis-induced DKA can be temporary and these patients might not necessarily require insulin upon discharge. Therefore, careful discharge planning is very important in such patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
