Kathleen R. Ruddiman DO , Catherine E. Price MD, ECNU, FACE , Alexander K. Bonnecaze MD
{"title":"A Case of Severe Cushing Syndrome due to Metastatic Adrenocortical Carcinoma Treated With Osilodrostat","authors":"Kathleen R. Ruddiman DO , Catherine E. Price MD, ECNU, FACE , Alexander K. Bonnecaze MD","doi":"10.1016/j.aace.2024.10.005","DOIUrl":null,"url":null,"abstract":"<div><h3>Background/Objective</h3><div>Osilodrostat used with block-and-replace dosing regimen is an off-label alternative to traditional management of Cushing syndrome due to adrenocortical carcinoma (ACC).</div></div><div><h3>Case Report</h3><div>A 70-year-old woman presented with abdominal pain and was found to have a large right adrenal mass and hypercortisolism. Right adrenalectomy was pursued with pathology consistent with diagnosis of ACC. Three months after surgery, hypercortisolemia recurred and bony metastatic disease was detected soon after. The patient received chemotherapy and mitotane; however, mitotane was stopped after development of hemolytic anemia. The patient’s urinary free cortisol became severely elevated, and osilodrostat was subsequently initiated for steroidogenesis inhibition. As dosage was increased, the patient presented with fatigue and hypotension and was diagnosed with adrenal insufficiency. This was managed with hydrocortisone in a block-and-replace dosing strategy.</div></div><div><h3>Discussion</h3><div>ACC can cause severe hypercortisolism, which is associated with significant morbidity and mortality. Osilodrostat was an effective off-label option for steroidogenesis inhibition in our patient who developed severe hypercortisolism and did not tolerate first-line therapy. Our patient also experienced iatrogenic adrenal insufficiency during treatment with osilodrostat, which was successfully managed using a block-and-replace strategy. There are limited cases currently available that document use of osilodrostat under the above circumstances.</div></div><div><h3>Conclusion</h3><div>Although osilodrostat is currently only approved for use in pituitary Cushing disease, we found it effective in off-label use to treat Cushing syndrome due to ACC. Using a block-and-replace treatment strategy was a practical intervention after development of adrenal insufficiency.</div></div>","PeriodicalId":7051,"journal":{"name":"AACE Clinical Case Reports","volume":"11 1","pages":"Pages 53-57"},"PeriodicalIF":1.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784602/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AACE Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2376060524001147","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background/Objective
Osilodrostat used with block-and-replace dosing regimen is an off-label alternative to traditional management of Cushing syndrome due to adrenocortical carcinoma (ACC).
Case Report
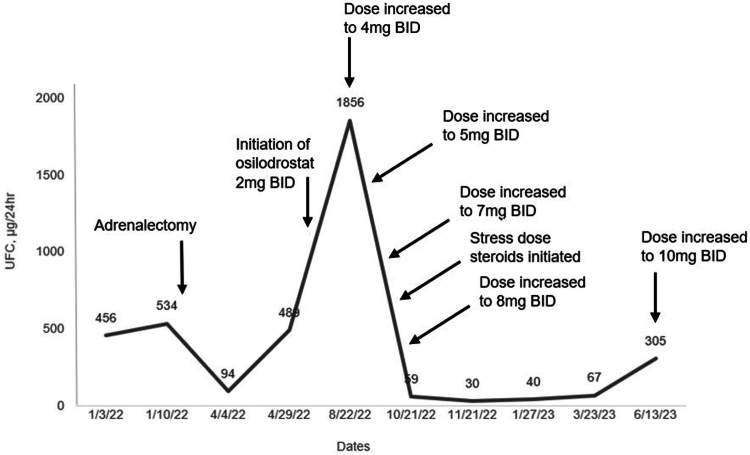
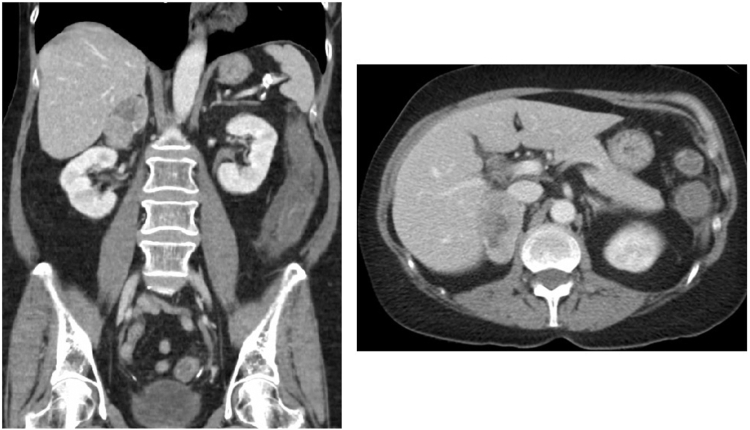
A 70-year-old woman presented with abdominal pain and was found to have a large right adrenal mass and hypercortisolism. Right adrenalectomy was pursued with pathology consistent with diagnosis of ACC. Three months after surgery, hypercortisolemia recurred and bony metastatic disease was detected soon after. The patient received chemotherapy and mitotane; however, mitotane was stopped after development of hemolytic anemia. The patient’s urinary free cortisol became severely elevated, and osilodrostat was subsequently initiated for steroidogenesis inhibition. As dosage was increased, the patient presented with fatigue and hypotension and was diagnosed with adrenal insufficiency. This was managed with hydrocortisone in a block-and-replace dosing strategy.
Discussion
ACC can cause severe hypercortisolism, which is associated with significant morbidity and mortality. Osilodrostat was an effective off-label option for steroidogenesis inhibition in our patient who developed severe hypercortisolism and did not tolerate first-line therapy. Our patient also experienced iatrogenic adrenal insufficiency during treatment with osilodrostat, which was successfully managed using a block-and-replace strategy. There are limited cases currently available that document use of osilodrostat under the above circumstances.
Conclusion
Although osilodrostat is currently only approved for use in pituitary Cushing disease, we found it effective in off-label use to treat Cushing syndrome due to ACC. Using a block-and-replace treatment strategy was a practical intervention after development of adrenal insufficiency.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
