{"title":"Development and Validation of a Scoring System to Predict 2-Year Clinical Remission in Ulcerative Colitis Patients on Vedolizumab.","authors":"Thanaboon Chaemsupaphan, Aviv Pudipeddi, Huiyu Lin, Sudarshan Paramsothy, Viraj Kariyawasam, Melissa Kermeen, Rupert W Leong","doi":"10.1093/crocol/otae068","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Vedolizumab is s gut-selective advanced therapy that is safe and efficacious for the treatment of ulcerative colitis (UC). Once patients achieve successful induction, there is a risk of loss of response leading to eventual flare. We aimed to identify these predictive factors and develop a practical scoring system to determine the ongoing efficacy of vedolizumab.</p><p><strong>Methods: </strong>We performed logistic regression on prospectively recruited UC subjects from the Vedolizumab Immunomodulator Enforced Withdrawal Study (VIEWS). All patients were in corticosteroid-free clinical remission and endoscopic improvement at baseline and continued vedolizumab. Predictive factors of 2-year corticosteroid-free clinical remission were determined and modeled into the VIEWS score, then validated in a real-world UC cohort.</p><p><strong>Results: </strong>Of 62 patients in the derivation cohort, 48 (77.4%) maintained clinical remission over two years. The predictive factors of remission were female (odds ratio [OR] 6.0, 95% confidence interval [CI], 1.2-29.7), antitumor necrosis factor naive (OR 3.8, 95% CI,1.0-14.0), baseline histological remission (OR 10.8, 95% CI, 2.4-48.4), thiopurine combination (OR 3.6, 95% CI, 0.7-18.0), and fecal calprotectin level ≤250 µg/g (OR 6.3, 95% CI, 0.9-42.2). These factors were incorporated into VIEWS score, yielding an area under the receiver-operating characteristic (AUROC) curve of 0.89 (95% CI, 0.81-0.98) in the prediction of 2-year clinical remission. Of 64 UC patients in the validation cohort, 40 (62.5%) remained in clinical remission at 2 years with AUROC of 0.77 (95% CI, 0.60-0.94). At the cut-off threshold of 4, the VIEWS score identified 2-year clinical remission with a sensitivity of 88.4% and specificity of 63.6%.</p><p><strong>Conclusions: </strong>Our study determined predictive factors and proposed a scoring system of ongoing clinical remission in UC patients on maintenance vedolizumab. In patients at high risk of relapse, combination therapy with thiopurine may be beneficial.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"7 1","pages":"otae068"},"PeriodicalIF":1.8000,"publicationDate":"2024-12-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11700619/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otae068","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Vedolizumab is s gut-selective advanced therapy that is safe and efficacious for the treatment of ulcerative colitis (UC). Once patients achieve successful induction, there is a risk of loss of response leading to eventual flare. We aimed to identify these predictive factors and develop a practical scoring system to determine the ongoing efficacy of vedolizumab.
Methods: We performed logistic regression on prospectively recruited UC subjects from the Vedolizumab Immunomodulator Enforced Withdrawal Study (VIEWS). All patients were in corticosteroid-free clinical remission and endoscopic improvement at baseline and continued vedolizumab. Predictive factors of 2-year corticosteroid-free clinical remission were determined and modeled into the VIEWS score, then validated in a real-world UC cohort.
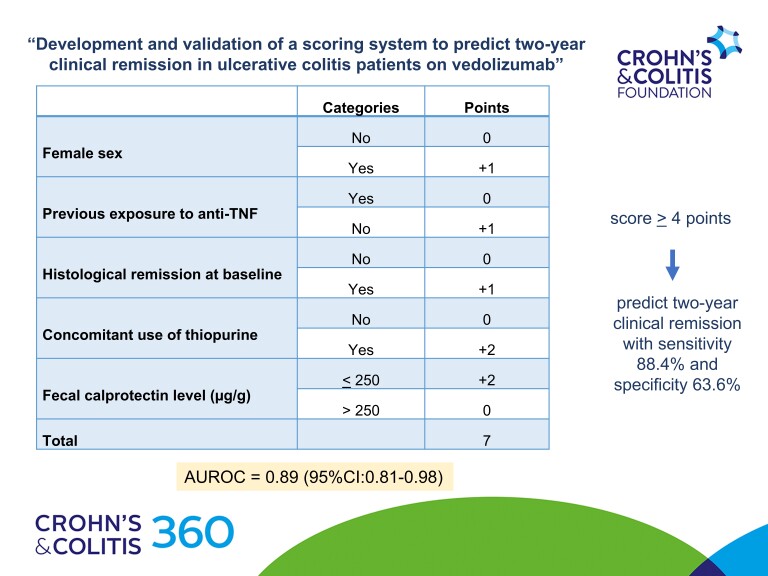
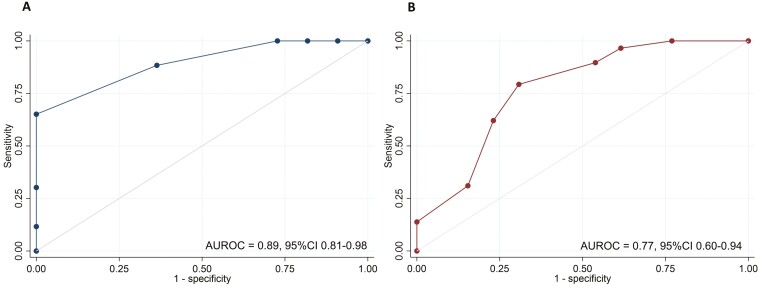
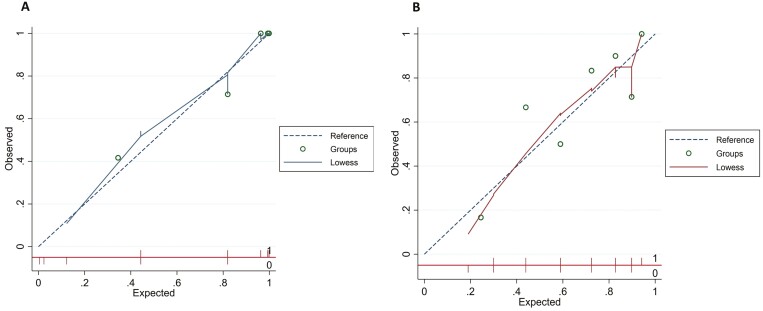
Results: Of 62 patients in the derivation cohort, 48 (77.4%) maintained clinical remission over two years. The predictive factors of remission were female (odds ratio [OR] 6.0, 95% confidence interval [CI], 1.2-29.7), antitumor necrosis factor naive (OR 3.8, 95% CI,1.0-14.0), baseline histological remission (OR 10.8, 95% CI, 2.4-48.4), thiopurine combination (OR 3.6, 95% CI, 0.7-18.0), and fecal calprotectin level ≤250 µg/g (OR 6.3, 95% CI, 0.9-42.2). These factors were incorporated into VIEWS score, yielding an area under the receiver-operating characteristic (AUROC) curve of 0.89 (95% CI, 0.81-0.98) in the prediction of 2-year clinical remission. Of 64 UC patients in the validation cohort, 40 (62.5%) remained in clinical remission at 2 years with AUROC of 0.77 (95% CI, 0.60-0.94). At the cut-off threshold of 4, the VIEWS score identified 2-year clinical remission with a sensitivity of 88.4% and specificity of 63.6%.
Conclusions: Our study determined predictive factors and proposed a scoring system of ongoing clinical remission in UC patients on maintenance vedolizumab. In patients at high risk of relapse, combination therapy with thiopurine may be beneficial.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
