M. Klein , H. Pirzadah , Y. Magharehabed , A. Chapple , N. Nair , A. Jernigan , T. Castellano
{"title":"“Developing a manual clinical trials screening process in a diverse southern gynecologic oncology practice”","authors":"M. Klein , H. Pirzadah , Y. Magharehabed , A. Chapple , N. Nair , A. Jernigan , T. Castellano","doi":"10.1016/j.gore.2024.101549","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>There is no standard clinical trial screening process in gynecologic oncology. In our low resource, highly diverse gynecologic oncology patient population, we sought to create an equitable, adaptable, manual screening process.</div></div><div><h3>Methods</h3><div>Our objective is to describe our clinical trial screening process and success in improving trial enrollment. An Institutional Review Board (IRB) approved quality improvement (QI) project was implemented in July 2022 to evaluate trial access. Screenable events were defined. Potential patients were those with a screenable event: new patients or diagnoses, regimen changes, progressions, and recurrences. Events were categorized into screen positive or screened no trial available. Screen positives were further categorized as screen positive, enrollment failure events or enrollments. Data about patients were collected via weekly research team meetings. Monthly meetings occurred to review progress. The data were compared to trials available, number of patients with trail available, and those that enrolled. Reasons for enrollment fails were tracked.</div></div><div><h3>Results</h3><div>Over time, “screen no trial available” (SNTA) rates stayed stable, but enrollment rates increased. Patient preference accounted for 32.8 % of enrollment failures (n = 42), pre-existing symptoms 23.4 % (n = 30), and location 21.1 % (n = 27). During increased employee turnover, there was a rise in enrollment fails due to staffing (n = 6, 4.7 %). We describe an effective process of clearly defining and tracking our patient population and ‘screenable events’ for which all patients are screened and offered trial participation if eligible.</div></div><div><h3>Conclusions</h3><div>We show that we improved understanding of the patient population, built a clinical trial portfolio better matched to population served, exceeded national averages for enrolling patients on trials, and are improving number eligible.</div></div>","PeriodicalId":12873,"journal":{"name":"Gynecologic Oncology Reports","volume":"57 ","pages":"Article 101549"},"PeriodicalIF":1.3000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11699326/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecologic Oncology Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2352578924002285","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
There is no standard clinical trial screening process in gynecologic oncology. In our low resource, highly diverse gynecologic oncology patient population, we sought to create an equitable, adaptable, manual screening process.
Methods
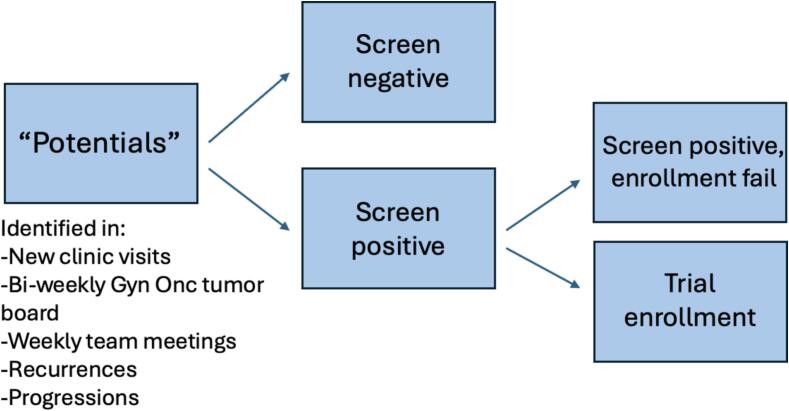
Our objective is to describe our clinical trial screening process and success in improving trial enrollment. An Institutional Review Board (IRB) approved quality improvement (QI) project was implemented in July 2022 to evaluate trial access. Screenable events were defined. Potential patients were those with a screenable event: new patients or diagnoses, regimen changes, progressions, and recurrences. Events were categorized into screen positive or screened no trial available. Screen positives were further categorized as screen positive, enrollment failure events or enrollments. Data about patients were collected via weekly research team meetings. Monthly meetings occurred to review progress. The data were compared to trials available, number of patients with trail available, and those that enrolled. Reasons for enrollment fails were tracked.
Results
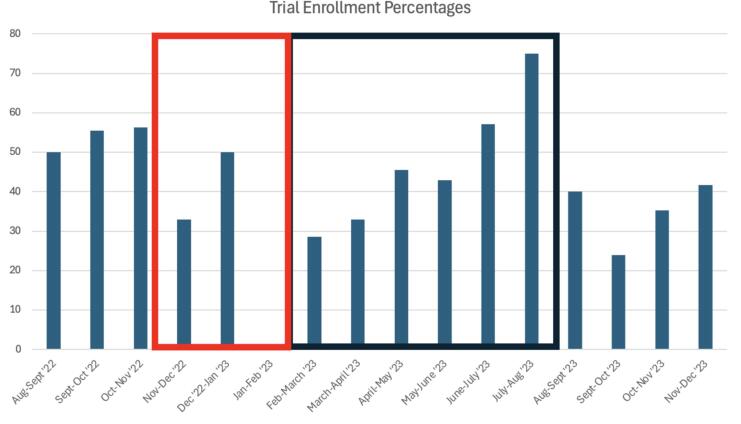
Over time, “screen no trial available” (SNTA) rates stayed stable, but enrollment rates increased. Patient preference accounted for 32.8 % of enrollment failures (n = 42), pre-existing symptoms 23.4 % (n = 30), and location 21.1 % (n = 27). During increased employee turnover, there was a rise in enrollment fails due to staffing (n = 6, 4.7 %). We describe an effective process of clearly defining and tracking our patient population and ‘screenable events’ for which all patients are screened and offered trial participation if eligible.
Conclusions
We show that we improved understanding of the patient population, built a clinical trial portfolio better matched to population served, exceeded national averages for enrolling patients on trials, and are improving number eligible.
期刊介绍:
Gynecologic Oncology Reports is an online-only, open access journal devoted to the rapid publication of narrative review articles, survey articles, case reports, case series, letters to the editor regarding previously published manuscripts and other short communications in the field of gynecologic oncology. The journal will consider papers that concern tumors of the female reproductive tract, with originality, quality, and clarity the chief criteria of acceptance.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
