Chu Luan Nguyen, Nirmal Dayaratna, Neshanth Easwaralingam, Jue Li Seah, Farhad Azimi, Cindy Mak, Carlo Pulitano, Sanjay Kumar Warrier
{"title":"Developing an Indocyanine Green Angiography Protocol for Predicting Flap Necrosis During Breast Reconstruction.","authors":"Chu Luan Nguyen, Nirmal Dayaratna, Neshanth Easwaralingam, Jue Li Seah, Farhad Azimi, Cindy Mak, Carlo Pulitano, Sanjay Kumar Warrier","doi":"10.1177/15533506241313172","DOIUrl":null,"url":null,"abstract":"<p><p>BackgroundAlthough there is evidence that indocyanine green angiography (ICGA) can predict mastectomy skin flap necrosis during breast reconstruction, consensus on optimal protocol is lacking. This study aimed to evaluate various technical factors which can influence ICG fluorescence intensity and thus interpretation of angiograms.MethodSingle institution retrospective study (2015-2021) of immediate implant-based breast reconstructions postmastectomy using a standardized technique of ICGA, controlling for modifiable factors of ambient lighting, camera distance and ICG dose. \"Time to perfusion\" assessment was defined as elapsed time from ICG administration to perfusion assessment. Intraoperative \"absolute\" and \"relative\" IGCA perfusion values of mastectomy flaps, taken at different time points (30, 60 and 90 seconds), were correlated with postoperative flap outcomes.ResultsThere were 260 breast reconstructions with a 3.1% necrosis rate. ICGA perfusion values, when measured at 60 and 90 seconds, were significantly lower for cases that developed necrosis compared to cases that did not, and were both good predictors of necrosis (area under ROC curves, 0.84 and 0.85, respectively). Fluorescence intensity increased as \"time to perfusion\" assessment increased for flaps that did not develop necrosis (correlation coefficient, 0.9, <i>P</i> < 0.001). Perfusion value cut-off thresholds for predicting necrosis were higher for a longer \"time to perfusion\" assessment.ConclusionsA standardized ICGA protocol is recommended as ICG fluorescence intensity increased with \"time to perfusion\" assessment, and ≤30 seconds did not allow for accurate perfusion analysis. Using a perfusion recording of 60 or 90 seconds, and the corresponding perfusion value cut-off, may optimize reliability of perfusion assessments.</p>","PeriodicalId":22095,"journal":{"name":"Surgical Innovation","volume":" ","pages":"77-84"},"PeriodicalIF":1.6000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11894893/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Innovation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/15533506241313172","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/6 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
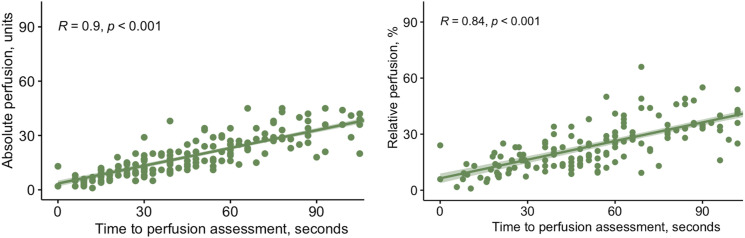
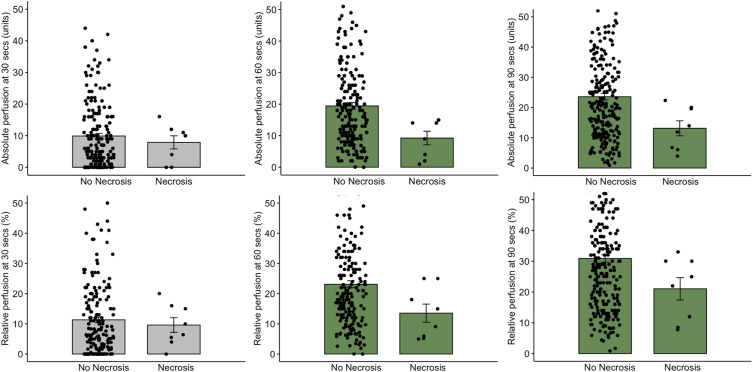
BackgroundAlthough there is evidence that indocyanine green angiography (ICGA) can predict mastectomy skin flap necrosis during breast reconstruction, consensus on optimal protocol is lacking. This study aimed to evaluate various technical factors which can influence ICG fluorescence intensity and thus interpretation of angiograms.MethodSingle institution retrospective study (2015-2021) of immediate implant-based breast reconstructions postmastectomy using a standardized technique of ICGA, controlling for modifiable factors of ambient lighting, camera distance and ICG dose. "Time to perfusion" assessment was defined as elapsed time from ICG administration to perfusion assessment. Intraoperative "absolute" and "relative" IGCA perfusion values of mastectomy flaps, taken at different time points (30, 60 and 90 seconds), were correlated with postoperative flap outcomes.ResultsThere were 260 breast reconstructions with a 3.1% necrosis rate. ICGA perfusion values, when measured at 60 and 90 seconds, were significantly lower for cases that developed necrosis compared to cases that did not, and were both good predictors of necrosis (area under ROC curves, 0.84 and 0.85, respectively). Fluorescence intensity increased as "time to perfusion" assessment increased for flaps that did not develop necrosis (correlation coefficient, 0.9, P < 0.001). Perfusion value cut-off thresholds for predicting necrosis were higher for a longer "time to perfusion" assessment.ConclusionsA standardized ICGA protocol is recommended as ICG fluorescence intensity increased with "time to perfusion" assessment, and ≤30 seconds did not allow for accurate perfusion analysis. Using a perfusion recording of 60 or 90 seconds, and the corresponding perfusion value cut-off, may optimize reliability of perfusion assessments.
期刊介绍:
Surgical Innovation (SRI) is a peer-reviewed bi-monthly journal focusing on minimally invasive surgical techniques, new instruments such as laparoscopes and endoscopes, and new technologies. SRI prepares surgeons to think and work in "the operating room of the future" through learning new techniques, understanding and adapting to new technologies, maintaining surgical competencies, and applying surgical outcomes data to their practices. This journal is a member of the Committee on Publication Ethics (COPE).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
