Stuart Campbell, Dane Hicks, Rajendra P Shetty, Bart J Currie
{"title":"Osteomyelitis and Septic Arthritis in the Darwin Prospective Melioidosis Study.","authors":"Stuart Campbell, Dane Hicks, Rajendra P Shetty, Bart J Currie","doi":"10.1093/ofid/ofae741","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Melioidosis is a multisystem infectious disease caused by the environmental bacterium <i>Burkholderia pseudomallei</i>. Osteomyelitis (OM) and septic arthritis (SA) are uncommon primary presentations for melioidosis but important secondary foci, often requiring prolonged therapy and multiple surgeries. We characterized the epidemiology, presentation, treatment, and outcomes of patients from 24 years of the Darwin Prospective Melioidosis Study (DPMS).</p><p><strong>Methods: </strong>DPMS patients from October 1, 1999, until September 30, 2023, were included if they had a primary or secondary diagnosis of OM or SA. Epidemiological, risk factor, clinical, and outcome data were retrieved from the DPMS database. Antibiotic and surgical data were collated from patient records.</p><p><strong>Results: </strong>From 1129 consecutive patients with culture-confirmed melioidosis, 122 (10.8%) had OM and/or SA, with 115 evaluable. Ninety-four of 1129 (8.3%) had OM, and 62/1129 (5.5%) had SA, with 41/115 (35.7%) of these having both OM and SA. Many combined infections involved contiguous bone and joints or soft tissue. Fifty-nine (51.3%) were male, and only 4.3% were ≤16 years old. Diabetes mellitus was present in 69.6%, and only 12.2% had no identifiable clinical risk factor. There were 8 deaths (7.0%) and 20 (17.4%) recurrent infections. Seventy-one (61.7%) had operative management, with combined infection associated with more procedures and longer length of stay.</p><p><strong>Conclusions: </strong>The current paradigm of care for osteoarticular melioidosis involves prolonged intravenous antibiotics in conjunction with timely and complete operative management, and in our setting where these are available, outcomes are good. In many melioidosis-endemic regions these resources are limited, and mortality remains high.</p>","PeriodicalId":19517,"journal":{"name":"Open Forum Infectious Diseases","volume":"12 1","pages":"ofae741"},"PeriodicalIF":3.8000,"publicationDate":"2024-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11697087/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Forum Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ofid/ofae741","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Melioidosis is a multisystem infectious disease caused by the environmental bacterium Burkholderia pseudomallei. Osteomyelitis (OM) and septic arthritis (SA) are uncommon primary presentations for melioidosis but important secondary foci, often requiring prolonged therapy and multiple surgeries. We characterized the epidemiology, presentation, treatment, and outcomes of patients from 24 years of the Darwin Prospective Melioidosis Study (DPMS).
Methods: DPMS patients from October 1, 1999, until September 30, 2023, were included if they had a primary or secondary diagnosis of OM or SA. Epidemiological, risk factor, clinical, and outcome data were retrieved from the DPMS database. Antibiotic and surgical data were collated from patient records.
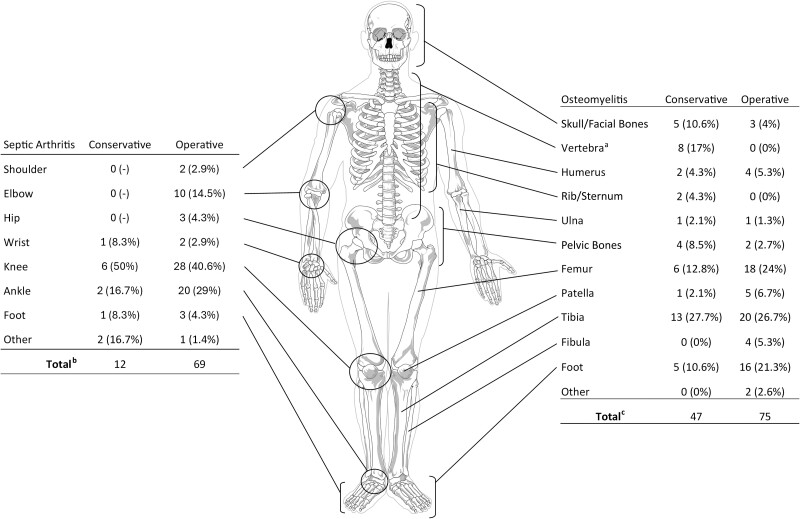
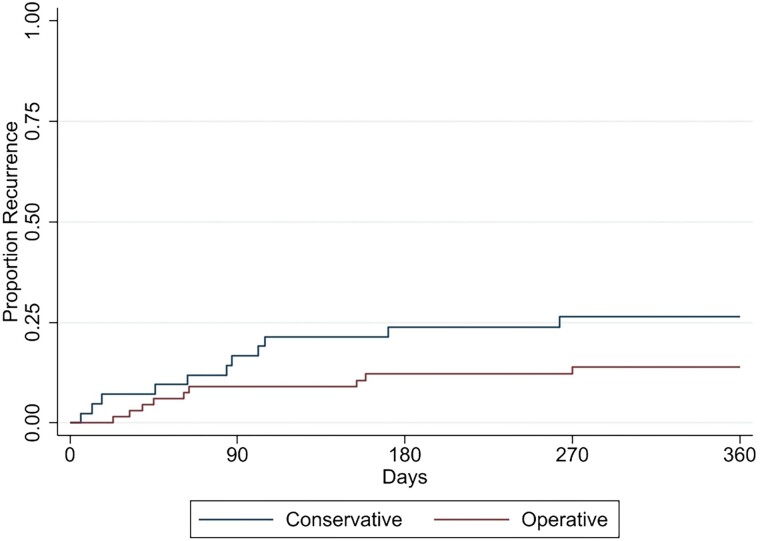
Results: From 1129 consecutive patients with culture-confirmed melioidosis, 122 (10.8%) had OM and/or SA, with 115 evaluable. Ninety-four of 1129 (8.3%) had OM, and 62/1129 (5.5%) had SA, with 41/115 (35.7%) of these having both OM and SA. Many combined infections involved contiguous bone and joints or soft tissue. Fifty-nine (51.3%) were male, and only 4.3% were ≤16 years old. Diabetes mellitus was present in 69.6%, and only 12.2% had no identifiable clinical risk factor. There were 8 deaths (7.0%) and 20 (17.4%) recurrent infections. Seventy-one (61.7%) had operative management, with combined infection associated with more procedures and longer length of stay.
Conclusions: The current paradigm of care for osteoarticular melioidosis involves prolonged intravenous antibiotics in conjunction with timely and complete operative management, and in our setting where these are available, outcomes are good. In many melioidosis-endemic regions these resources are limited, and mortality remains high.
期刊介绍:
Open Forum Infectious Diseases provides a global forum for the publication of clinical, translational, and basic research findings in a fully open access, online journal environment. The journal reflects the broad diversity of the field of infectious diseases, and focuses on the intersection of biomedical science and clinical practice, with a particular emphasis on knowledge that holds the potential to improve patient care in populations around the world. Fully peer-reviewed, OFID supports the international community of infectious diseases experts by providing a venue for articles that further the understanding of all aspects of infectious diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
