Jad G. Khalil , Eeric Truumees , Kevin Macadaeg , Daniel T.D. Nguyen , Gregory A. Moore , Dylan Lukes , Jeffrey Fischgrund
{"title":"Intraosseous basivertebral nerve ablation: A 5-year pooled analysis from three prospective clinical trials","authors":"Jad G. Khalil , Eeric Truumees , Kevin Macadaeg , Daniel T.D. Nguyen , Gregory A. Moore , Dylan Lukes , Jeffrey Fischgrund","doi":"10.1016/j.inpm.2024.100529","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Vertebrogenic pain is a documented source of anterior column chronic low back pain (CLBP) that stems from damaged vertebral endplates. Nociceptive signals are transmitted by the basivertebral nerve (BVN) and endplate damage is observed as Type 1 or Type 2 Modic changes (MC) on magnetic resonance imaging (MRI). The clinical impact and safety of intraosseous radiofrequency ablation of the BVN (BVNA) for the treatment of vertebrogenic pain has been demonstrated in three prospective clinical trials (two randomized and one single-arm study).</div></div><div><h3>Objective</h3><div>Report aggregate long-term BVNA outcomes at five years from three studies.</div></div><div><h3>Methods</h3><div>Pooled results at 5-years post-BVNA are reported for three clinical trials with similar inclusion/exclusion criteria and outcomes measurements: 1) a prospective, open label, single-arm follow-up of the treatment arm of a randomized controlled trial (RCT) comparing BVNA to sham ablation (SMART); 2) a prospective, open label, single-arm follow-up of the treatment arm of an RCT comparing BVNA to standard care (INTRACEPT); and 3) a prospective, open label, single-arm long-term follow-up study of BVNA-treated participants (CLBP Single-Arm). Paired datasets (baseline and 5-years) for mean changes in Oswestry disability index (ODI) and numeric pain scores (NPS) were analyzed using a two-sided paired <em>t</em>-test with a 0.05 level of significance. Secondary outcomes included responder rates, patient satisfaction, adverse events, and healthcare utilization.</div></div><div><h3>Results</h3><div>Two hundred forty-nine (249) of 320 BVNA-treated participants (78 % participation rate) completed a five-year visit (mean of 5.6 years follow-up). At baseline, 71.9 % of these participants reported back pain for ≥5 years, 27.7 % were taking opioids, and 61.8 % had prior therapeutic lumbar spinal injections. Pain and functional improvements were significant at 5-years with a mean improvement in NPS of 4.32 ± 2.45 points (95 % CI 4.01, 4.63; p < 0.0001) from 6.79 ± 1.32 at baseline and a mean improvement in ODI of 28.0 ± 17.5 (95 % CI 25.8, 30.2; p < 0.0001) from 44.5 ± 11.0 at baseline. Nearly one-third (32.1 %) of patients reported being pain-free (NPS = 0) at five years, 72.7 % of patients indicated their condition improved and 68.7 % had resumed activity levels they had prior to onset of CLBP. In the sixty-nine participants taking opioids at baseline, 65.2 % were no longer taking them at 5-years, and spinal injections decreased by 58.1 %. The rate of lumbosacral treatment (therapeutic spinal injection, radiofrequency ablation, or surgery) for the same index pain source and vertebral level was 33/249 (13.2 %) at 5 years post BVNA; including a 6.0 % rate of lumbar fusion. There were no serious device or device-procedure related adverse events reported during the long-term follow-up.</div></div><div><h3>Conclusion</h3><div>In this 5-year aggregate analysis, BVNA significantly improved pain and function scores compared to baseline. Similarly, there were significant reductions in opioid consumption and spinal injections post BVNA. Data demonstrate a strong safety profile with no serious device or device-related events and low healthcare utilization rate for the same index pain source through a mean of 5.6 years. Results demonstrate that intraosseous BVNA treatment for patients with vertebrogenic pain is safe, effective, and durable through five years.</div></div>","PeriodicalId":100727,"journal":{"name":"Interventional Pain Medicine","volume":"3 4","pages":"Article 100529"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11700295/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interventional Pain Medicine","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S277259442400150X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/13 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Vertebrogenic pain is a documented source of anterior column chronic low back pain (CLBP) that stems from damaged vertebral endplates. Nociceptive signals are transmitted by the basivertebral nerve (BVN) and endplate damage is observed as Type 1 or Type 2 Modic changes (MC) on magnetic resonance imaging (MRI). The clinical impact and safety of intraosseous radiofrequency ablation of the BVN (BVNA) for the treatment of vertebrogenic pain has been demonstrated in three prospective clinical trials (two randomized and one single-arm study).
Objective
Report aggregate long-term BVNA outcomes at five years from three studies.
Methods
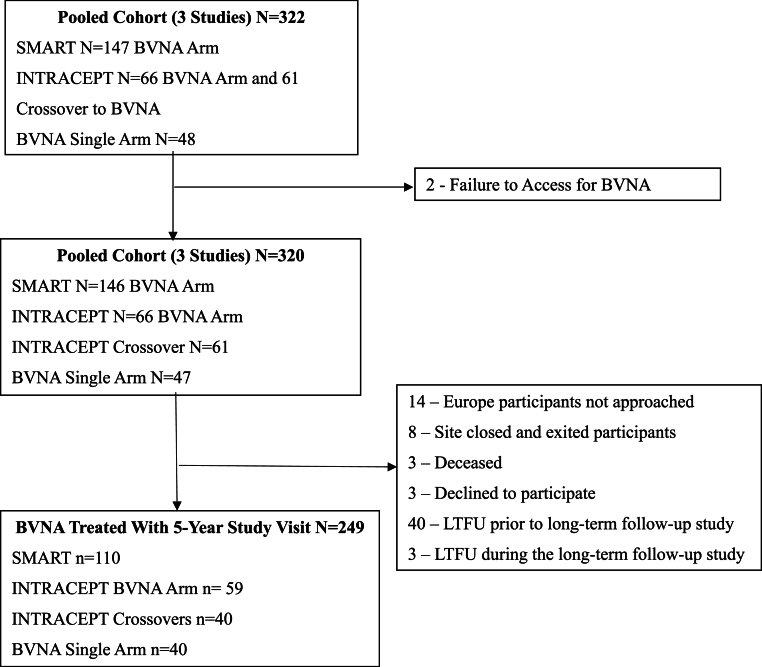
Pooled results at 5-years post-BVNA are reported for three clinical trials with similar inclusion/exclusion criteria and outcomes measurements: 1) a prospective, open label, single-arm follow-up of the treatment arm of a randomized controlled trial (RCT) comparing BVNA to sham ablation (SMART); 2) a prospective, open label, single-arm follow-up of the treatment arm of an RCT comparing BVNA to standard care (INTRACEPT); and 3) a prospective, open label, single-arm long-term follow-up study of BVNA-treated participants (CLBP Single-Arm). Paired datasets (baseline and 5-years) for mean changes in Oswestry disability index (ODI) and numeric pain scores (NPS) were analyzed using a two-sided paired t-test with a 0.05 level of significance. Secondary outcomes included responder rates, patient satisfaction, adverse events, and healthcare utilization.
Results
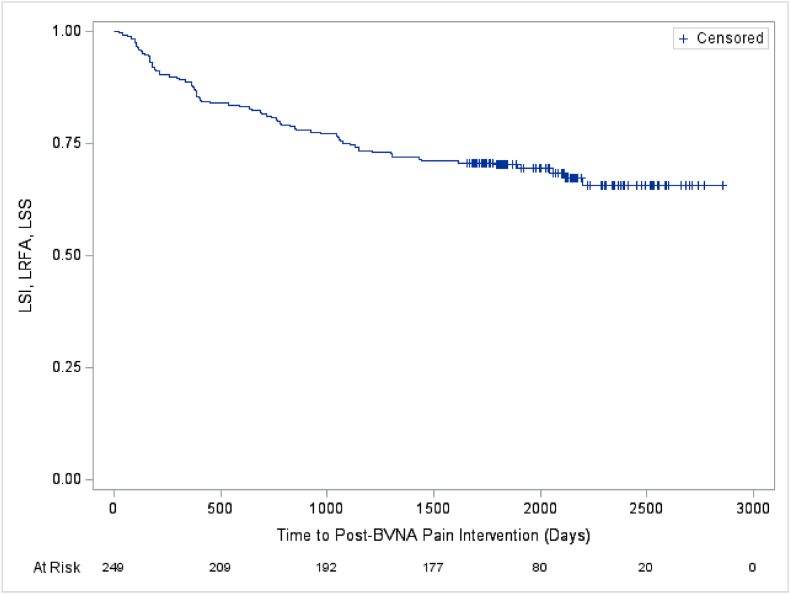
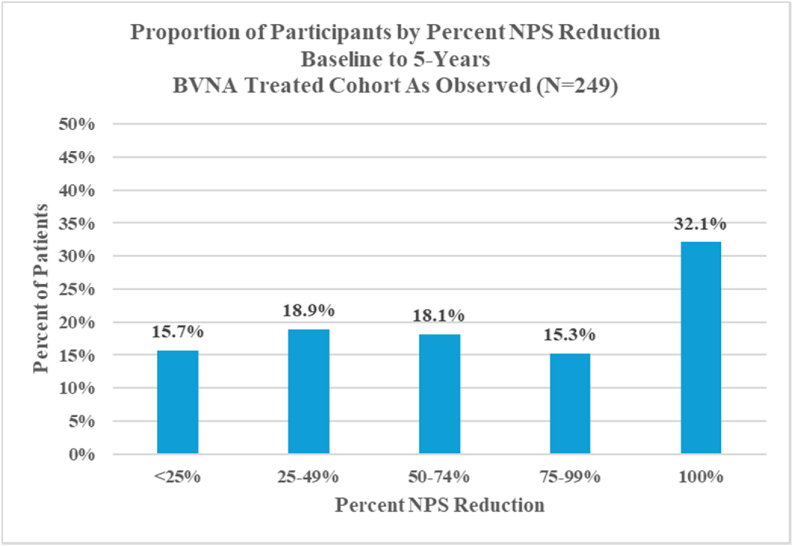
Two hundred forty-nine (249) of 320 BVNA-treated participants (78 % participation rate) completed a five-year visit (mean of 5.6 years follow-up). At baseline, 71.9 % of these participants reported back pain for ≥5 years, 27.7 % were taking opioids, and 61.8 % had prior therapeutic lumbar spinal injections. Pain and functional improvements were significant at 5-years with a mean improvement in NPS of 4.32 ± 2.45 points (95 % CI 4.01, 4.63; p < 0.0001) from 6.79 ± 1.32 at baseline and a mean improvement in ODI of 28.0 ± 17.5 (95 % CI 25.8, 30.2; p < 0.0001) from 44.5 ± 11.0 at baseline. Nearly one-third (32.1 %) of patients reported being pain-free (NPS = 0) at five years, 72.7 % of patients indicated their condition improved and 68.7 % had resumed activity levels they had prior to onset of CLBP. In the sixty-nine participants taking opioids at baseline, 65.2 % were no longer taking them at 5-years, and spinal injections decreased by 58.1 %. The rate of lumbosacral treatment (therapeutic spinal injection, radiofrequency ablation, or surgery) for the same index pain source and vertebral level was 33/249 (13.2 %) at 5 years post BVNA; including a 6.0 % rate of lumbar fusion. There were no serious device or device-procedure related adverse events reported during the long-term follow-up.
Conclusion
In this 5-year aggregate analysis, BVNA significantly improved pain and function scores compared to baseline. Similarly, there were significant reductions in opioid consumption and spinal injections post BVNA. Data demonstrate a strong safety profile with no serious device or device-related events and low healthcare utilization rate for the same index pain source through a mean of 5.6 years. Results demonstrate that intraosseous BVNA treatment for patients with vertebrogenic pain is safe, effective, and durable through five years.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
