Maor Tzuberi, Rafael Y Brzezinski, Nir Flint, Moaad Slieman, Lior Zornitzki, Dana Viskin, Anna Rozenfeld Hemed, Barliz Waissengrin, Renana Barak, Inbal Golomb, Ido Wolf, Netanel Golan, Yan Topilsky, Shmuel Banai, Livia Kapusta, Michal Laufer-Perl
{"title":"Safety and efficacy of immune checkpoint inhibitors in patients with pre-treatment reduced left ventricular function.","authors":"Maor Tzuberi, Rafael Y Brzezinski, Nir Flint, Moaad Slieman, Lior Zornitzki, Dana Viskin, Anna Rozenfeld Hemed, Barliz Waissengrin, Renana Barak, Inbal Golomb, Ido Wolf, Netanel Golan, Yan Topilsky, Shmuel Banai, Livia Kapusta, Michal Laufer-Perl","doi":"10.1186/s40959-024-00297-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment outcomes. However, the response varies across different populations, and their use may lead to life-threatening cardiovascular (CV) events. While pre-treatment reduced left ventricular ejection fraction (LVEF) is considered a marker for high-risk cardiotoxicity and a contraindication for anthracycline and HER2-targeted therapies, there is limited evidence on the safety and efficacy of ICIs therapy in patients presenting with pre-treatment reduced LVEF. The study aims to evaluate the safety and efficacy of ICIs therapy in patients with pre-treatment reduced LVEF.</p><p><strong>Methods: </strong>Retrospective single center cohort of patients treated with ICIs therapy, who performed pre-treatment LVEF assessment. The primary endpoint was to evaluate the safety of ICIs among this population, assessed by CV events (composite of myocarditis, acute coronary syndrome, heart failure, and arrhythmias). The secondary endpoint was to evaluate the efficacy of ICIs, assessed by all-cause mortality and progression-free survival (PFS).</p><p><strong>Results: </strong>The cohort included 307 patients, with 30 (10%) presenting with pre-treatment reduced LVEF, with a mean LVEF of 39 ± 7%. While a significantly higher incidence of CV events was observed in the reduced LVEF group (37% vs. 14%, p = 0.004), following a multivariate Cox regression analysis including baseline CV diseases and risk factors, pre-treatment reduced LVEF did not remain a significant independent predictor (p = 0.358). No significant differences were observed between the groups regarding all-cause mortality and PFS.</p><p><strong>Conclusions: </strong>Pre-treatment reduced LVEF was not identified as an independent marker for clinical outcomes in patients treated with ICIs therapy.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"2"},"PeriodicalIF":3.2000,"publicationDate":"2025-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11707996/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00297-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment outcomes. However, the response varies across different populations, and their use may lead to life-threatening cardiovascular (CV) events. While pre-treatment reduced left ventricular ejection fraction (LVEF) is considered a marker for high-risk cardiotoxicity and a contraindication for anthracycline and HER2-targeted therapies, there is limited evidence on the safety and efficacy of ICIs therapy in patients presenting with pre-treatment reduced LVEF. The study aims to evaluate the safety and efficacy of ICIs therapy in patients with pre-treatment reduced LVEF.
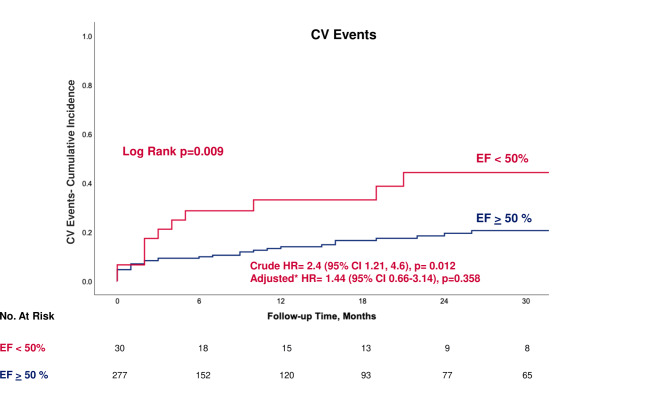
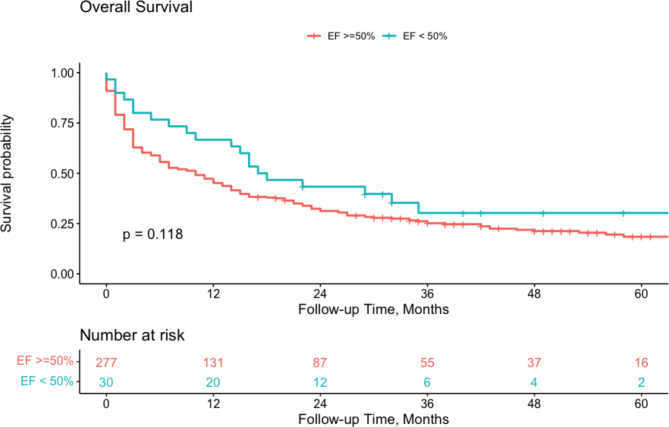
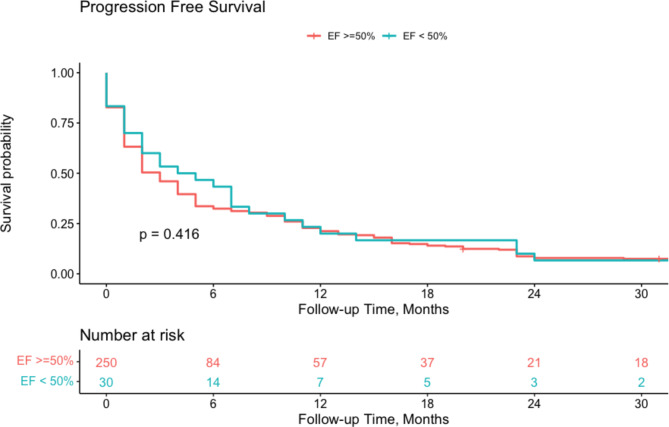
Methods: Retrospective single center cohort of patients treated with ICIs therapy, who performed pre-treatment LVEF assessment. The primary endpoint was to evaluate the safety of ICIs among this population, assessed by CV events (composite of myocarditis, acute coronary syndrome, heart failure, and arrhythmias). The secondary endpoint was to evaluate the efficacy of ICIs, assessed by all-cause mortality and progression-free survival (PFS).
Results: The cohort included 307 patients, with 30 (10%) presenting with pre-treatment reduced LVEF, with a mean LVEF of 39 ± 7%. While a significantly higher incidence of CV events was observed in the reduced LVEF group (37% vs. 14%, p = 0.004), following a multivariate Cox regression analysis including baseline CV diseases and risk factors, pre-treatment reduced LVEF did not remain a significant independent predictor (p = 0.358). No significant differences were observed between the groups regarding all-cause mortality and PFS.
Conclusions: Pre-treatment reduced LVEF was not identified as an independent marker for clinical outcomes in patients treated with ICIs therapy.
目的:免疫检查点抑制剂(ICIs)已经彻底改变了癌症的治疗结果。然而,不同人群的反应不同,它们的使用可能导致危及生命的心血管事件。虽然治疗前左室射血分数降低(LVEF)被认为是高危心脏毒性的标志,也是蒽环类药物和her2靶向治疗的禁忌症,但关于治疗前LVEF降低的患者使用ICIs治疗的安全性和有效性的证据有限。本研究旨在评价ICIs治疗前LVEF降低患者的安全性和有效性。方法:对接受ICIs治疗的患者进行回顾性单中心队列研究,并进行治疗前LVEF评估。主要终点是通过CV事件(心肌炎、急性冠状动脉综合征、心力衰竭和心律失常的组合)来评估ICIs在该人群中的安全性。次要终点是通过全因死亡率和无进展生存期(PFS)来评估ICIs的疗效。结果:该队列包括307例患者,其中30例(10%)表现为治疗前LVEF减少,平均LVEF为39±7%。在包括基线CV疾病和危险因素在内的多因素Cox回归分析后,虽然LVEF降低组的CV事件发生率明显较高(37% vs. 14%, p = 0.004),但治疗前LVEF降低并不是一个显著的独立预测因子(p = 0.358)。在全因死亡率和PFS方面,组间无显著差异。结论:治疗前降低的LVEF未被确定为接受ICIs治疗的患者临床结果的独立标志。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
