Moojun Kim, Chang-Ok Seo, Yong-Lee Kim, Hangyul Kim, Hye Ree Kim, Yun Ho Cho, Jeong Yoon Jang, Jong-Hwa Ahn, Min Gyu Kang, Kyehwan Kim, Jin-Sin Koh, Seok-Jae Hwang, Jin Yong Hwang, Jeong Rang Park
{"title":"Predictive value and optimal cut-off level of high-sensitivity troponin T in patients with acute pulmonary embolism.","authors":"Moojun Kim, Chang-Ok Seo, Yong-Lee Kim, Hangyul Kim, Hye Ree Kim, Yun Ho Cho, Jeong Yoon Jang, Jong-Hwa Ahn, Min Gyu Kang, Kyehwan Kim, Jin-Sin Koh, Seok-Jae Hwang, Jin Yong Hwang, Jeong Rang Park","doi":"10.3904/kjim.2024.131","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>Elevated troponin levels predict in-hospital mortality and influence decisions regarding thrombolytic therapy in patients with acute pulmonary embolism (PE). However, the usefulness of high-sensitivity troponin T (hsTnT) regarding PE remains uncertain. We aimed to establish the optimal cut-off level and compare its performance for precise risk stratification.</p><p><strong>Methods: </strong>374 patients diagnosed with acute PE were reviewed. PE-related adverse outcomes, a composite of PE-related deaths, cardiopulmonary resuscitation incidents, systolic blood pressure < 90 mmHg, and all-cause mortality within 30 days were evaluated. The optimal hsTnT cut-off for all-cause mortality, and the net reclassification index (NRI) was used to assess the incremental value in risk stratification.</p><p><strong>Results: </strong>Among 343 normotensive patients, 17 (5.0%) experienced all-cause mortality, while 40 (10.7%) had PE-related adverse outcomes. An optimal hsTnT cut-off value of 60 ng/L for all-cause mortality (AUC 0.74, 95% CI 0.61-0.85, p < 0.001) was identified, which was significantly associated with PE-related adverse outcomes (OR 4.07, 95% CI 2.06-8.06, p < 0.001). Patients with hsTnT ≥ 60 ng/L were older, hypotensive, had higher creatinine levels, and right ventricular dysfunction signs. Combining hsTnT ≥ 60 ng/L with simplified pulmonary embolism severity index ≥1 provided additional prognostic information. Reclassification analysis showed a significant shift in risk categories, with an NRI of 1.016 ± 0.201 (p < 0.001).</p><p><strong>Conclusion: </strong>We refined troponin's predictive value in patients with acute PE, proposing a new cut-off value of hsTnT ≥ 60 ng/L. Validation through large-scale studies is essential to offer clinically useful guidance for managing patient population.</p>","PeriodicalId":48785,"journal":{"name":"Korean Journal of Internal Medicine","volume":"40 1","pages":"65-77"},"PeriodicalIF":2.4000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11725470/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3904/kjim.2024.131","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aims: Elevated troponin levels predict in-hospital mortality and influence decisions regarding thrombolytic therapy in patients with acute pulmonary embolism (PE). However, the usefulness of high-sensitivity troponin T (hsTnT) regarding PE remains uncertain. We aimed to establish the optimal cut-off level and compare its performance for precise risk stratification.
Methods: 374 patients diagnosed with acute PE were reviewed. PE-related adverse outcomes, a composite of PE-related deaths, cardiopulmonary resuscitation incidents, systolic blood pressure < 90 mmHg, and all-cause mortality within 30 days were evaluated. The optimal hsTnT cut-off for all-cause mortality, and the net reclassification index (NRI) was used to assess the incremental value in risk stratification.
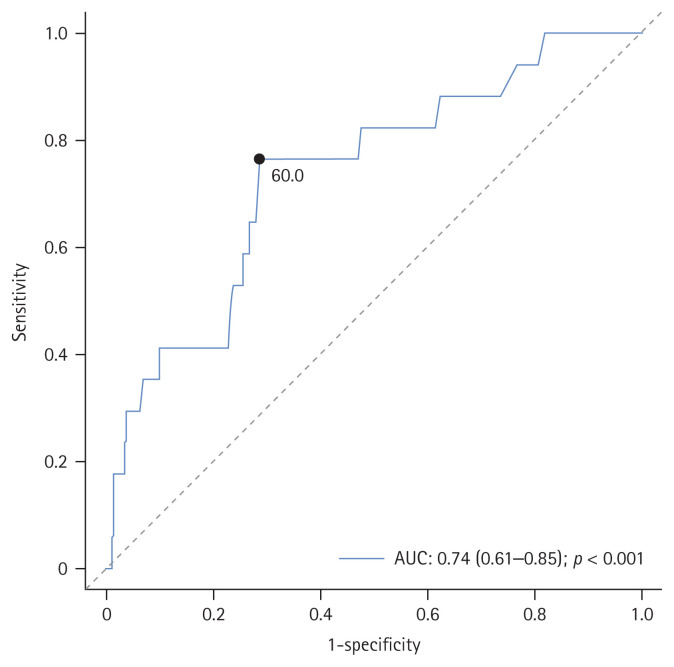
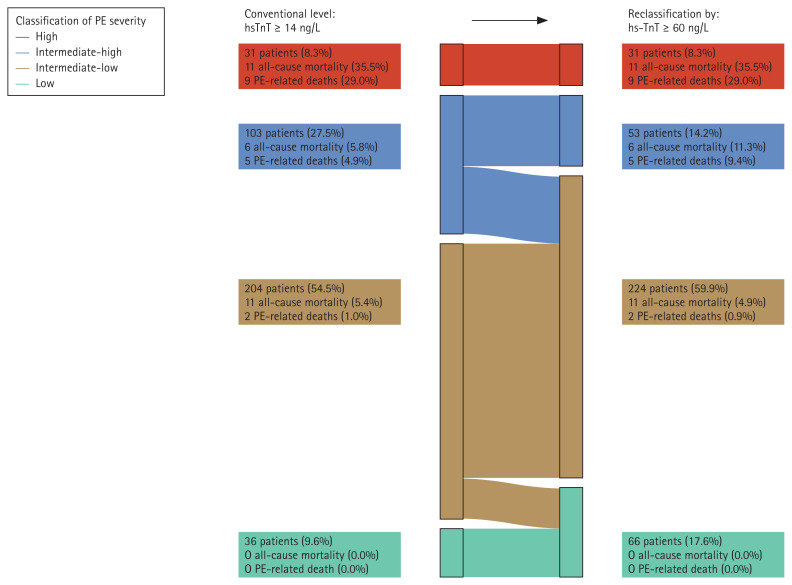
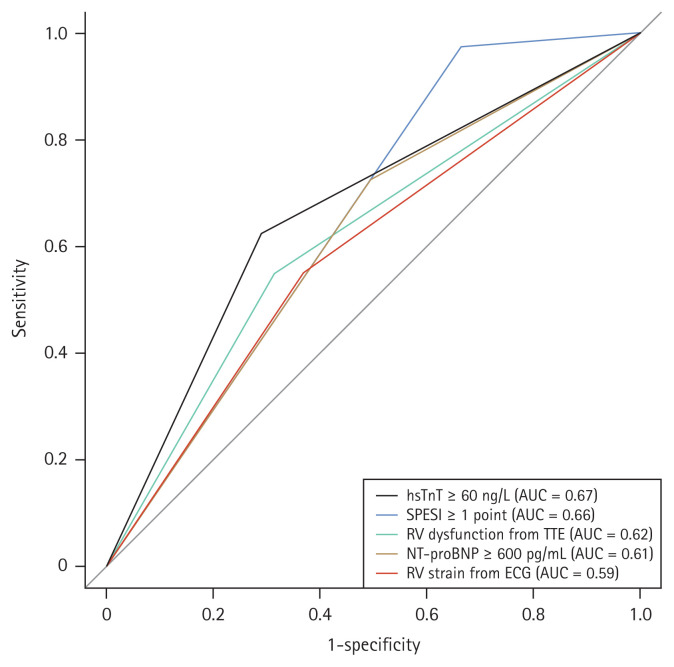
Results: Among 343 normotensive patients, 17 (5.0%) experienced all-cause mortality, while 40 (10.7%) had PE-related adverse outcomes. An optimal hsTnT cut-off value of 60 ng/L for all-cause mortality (AUC 0.74, 95% CI 0.61-0.85, p < 0.001) was identified, which was significantly associated with PE-related adverse outcomes (OR 4.07, 95% CI 2.06-8.06, p < 0.001). Patients with hsTnT ≥ 60 ng/L were older, hypotensive, had higher creatinine levels, and right ventricular dysfunction signs. Combining hsTnT ≥ 60 ng/L with simplified pulmonary embolism severity index ≥1 provided additional prognostic information. Reclassification analysis showed a significant shift in risk categories, with an NRI of 1.016 ± 0.201 (p < 0.001).
Conclusion: We refined troponin's predictive value in patients with acute PE, proposing a new cut-off value of hsTnT ≥ 60 ng/L. Validation through large-scale studies is essential to offer clinically useful guidance for managing patient population.
期刊介绍:
The Korean Journal of Internal Medicine is an international medical journal published in English by the Korean Association of Internal Medicine. The Journal publishes peer-reviewed original articles, reviews, and editorials on all aspects of medicine, including clinical investigations and basic research. Both human and experimental animal studies are welcome, as are new findings on the epidemiology, pathogenesis, diagnosis, and treatment of diseases. Case reports will be published only in exceptional circumstances, when they illustrate a rare occurrence of clinical importance. Letters to the editor are encouraged for specific comments on published articles and general viewpoints.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
